According to the American Pediatric Association, measles was eliminated in the United States in 2000, when there was a year without recording an endemic spread of the virus. Measles is a highly contagious virus. Only humans can spread and get measles. Measles outbreaks in the United States result from an infected person bringing measles into a community.
{kind=link}
Studies have shown that the quickest way to protect against measles is with the measles, mumps, and rubella (MMR) vaccine. Two doses of the MMR are about 97% effective in preventing measles and one dose is 93% effective in preventing measles.
Both children and adults can get the MMR vaccine.
Brief Overview:
This article:
- Provides information on why measles is beginning to spread again in the United States after several years with no community-wide infections
- Explains how “herd immunity” protection works and why it can stop working
- Describes the complications that can result from measles, including permanent conditions
- Includes the signs and symptoms of measles
- The quickest way to protect against measles is the Measles, Mumps, and Rubella (MMR) vaccine, which can be given to children and adults
Full Article:
Why are we talking about Measles? What is herd immunity?
According to the American Pediatric Association, measles was eliminated in the United States in 2000, when there was a year without recording an endemic spread of the virus. Measles outbreaks in the United States result from an infected person bringing measles into a community.
Measles outbreaks have happened in small pockets or communities of unvaccinated people in recent years. Within these communities the measles virus spreads quickly; without herd immunity, it is difficult to stop the outbreak. The COVID shutdown made it difficult for many families to vaccinate their children, and it has been a slow process to provide information on why vaccinations create safety barriers for children and families from disease. One of the most significant outbreaks in a while is happening this year (2025) in Texas and New Mexico and has shown up in 12 other states including Washington. Health officials are keeping an eye on the spread, and you can get information on cases in Washington State through the Washington State Health Department website.
This year was the first documented case of a death from measles in the U.S. in a decade. About 1 out of 5 unvaccinated people in the U.S. who get measles are hospitalized. Measles can have severe health complications: pneumonia, encephalitis (swelling of the brain), convulsions, and brain damage, resulting in possible deafness or an intellectual disability. One result of having measles can be a suppressed immune system lasting 2-3 years or longer. In addition, The MedlinePlus medical library of the National Institutes of Health states, “SSPE Subacute sclerosing panencephalitis (SSPE) is a progressive, disabling, and deadly brain disorder related to measles (rubeola) infection. SSPE is rarely seen in the United States since the implementation of the vaccination program.”
The United States was able to eliminate measles by having a high percentage of the population develop immunity by measles vaccination or natural immunity by having the virus known as herd immunity. Herd immunity is achieved when 95 percent of the population has developed immunity by contracting a virus or other disease or being vaccinated. In past years, the large number of people protected from the measles virus protected the few unprotected people from getting the virus. If they did get the virus, herd immunity keeps it from spreading. In the United States, by the year 2020, we had achieved zero percent cases of measles per every 100,000 people, or for all practical purposes, we had achieved 100% herd immunity.
How is the measles virus spread?
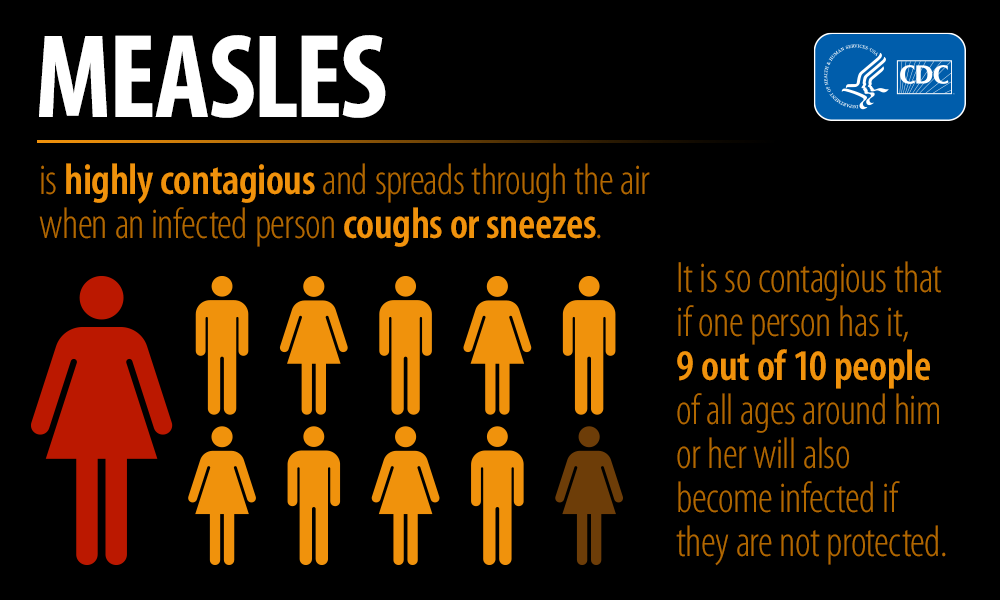
Measles is a highly contagious virus. Only humans can spread and get measles. Measles lives in the mucus of the nose and throat of an infected person. Measles can spread when a person coughs or sneezes in the air. If another person breathes in the contaminated droplets or by touching the infected surface, then touches their eyes, nose, or mouth, they can become infected. The virus can live in the air for up to 2 hours.
A person is infectious even before they know they have the disease. They can spread the disease up to four days before and four days after they have the rash.
Prevention
Studies have shown that the quickest way to protect against measles is with the measles, mumps, and rubella (MMR) vaccine. Two doses of the MMR are about 97% effective in preventing measles and one dose is 93% effective in preventing measles.
Both children and adults can get the MMR vaccine. This webpage on the Centers for Disease Control (CDC) website has information on who is recommended to get the vaccine, who should not get it, and where to get the vaccine and options for paying for it.
The Measles, Mumps and Rubella (MMR) vaccine is free to all infants and children in the United States, and you can request a vaccine for your child if they are unvaccinated, through their doctor or at a Community Health Clinic.
Seattle’s Children’s Hospital provides the following information on side effects from the vaccine shot.
- A mild fever of less than 103 degrees F. in 10% of children vaccinated lasting 2 or 3 days.
- A mild pink rash on the body’s trunk lasts 2 or 3 days. No treatment is needed. Your child can go to school or childcare with the rash.
It is recommended that caregivers call your doctor if:
- Rash changes to blood-colored spots.
- Rash lasts more than 3 days.
A lot has been shared about Vitamin A and measles across many avenues of information. It has been documented across the medical field in multiple medical journals and from various Children’s Hospitals that vitamin A cannot prevent a person from getting measles. Where Vitamin A has been most effective in the treatment of measles has been as a supplemental treatment that can be added in severe cases to reduce the risk of death for some children with a deficiency of Vitamin A in their system. Still, it does not prevent catching measles and can be toxic if a child or adult gets too much.
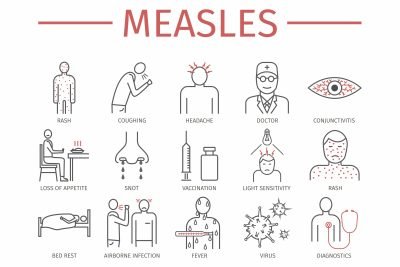
Signs and Symptoms of Measles
The first sign of measles symptoms appears 7-14 days after a measles infection. A person is contagious before showing any signs of the measles rash.
Measles usually begins with:
- A consistent high fever. (may peak at 104 degrees F)
- A cough
- Runny nose
- Red watery eyes
2-3 days after symptoms begin tiny white spots (Koplik spots) may appear inside the mouth.
The measles rash may start to appear 3-5 days after the initial onset of symptoms. The rash begins as flat red spots that begin on the face at the edge of the hairline. The rash spreads downward to the neck, trunk, arms, legs, and feet. Small, raised bumps may appear on top of the flat red spots. As the rash spreads across the body the spots may become joined together. When the rash appears a person’s fever may spike higher than 104 degrees F.
Common Complications from Measles
- Ear infections occur in one out of every ten children with measles.
- Diarrhea can occur with measles.
What to do if you think your child has measles
The CDC states, “Measles is not just a little rash. Measles can be dangerous, especially for babies and young children. If you suspect that you or your child has been exposed to the measles, call you healthcare provider immediately.”
Here are some additional links and resources:
Preventing Measles Before and After Travel Fact Sheet – also available for download in the following languages: Spanish, Russian, Ukrainian, Romanian, Amharic, Hindi, Somali, Arabic and Urdu.
A Measles facts sheet is provided by the Pediatric Pandemic Network that can be kept as a reference sheet and provides images of measles.
Seattle Children’s Hospital information on measles vaccine side effects
If you are planning international travel talk to your doctor. Here is an infographic link from the CDC you can click on and download to use for helpful tips. Protect your child from contracting measles.
{kind=link}
Here are some additional links and resources:
Center for Disease Control information provided about measles – Preventing Measles Before and After Travel Fact Sheet – also available for download in the following languages: Spanish, Russian, Ukrainian, Romanian, Amharic, Hindi, Somali, Arabic and Urdu.
Measles facts sheet is provided by the Pediatric Pandemic Network that can be kept as a reference sheet and provides images of measles.
Seattle Children’s Hospital information on measles vaccine side effects
If you are planning international travel talk to your doctor.
Protect your child from contracting measles. an infographic link from the CDC you can click on and download to use for helpful tips.