Families who enroll their child with disabilities in a private school keep important legal protections, though these are different from those in public schools. Public school districts are still responsible for evaluating (testing) a child for special education and may offer limited support through a services plan developed together with the family and the private school. Families who stay involved with both school systems serving their student, private and public, have the chance to ask for the services their child gets, even when a public school system has limited resources based on local priorities.
A Brief Overview
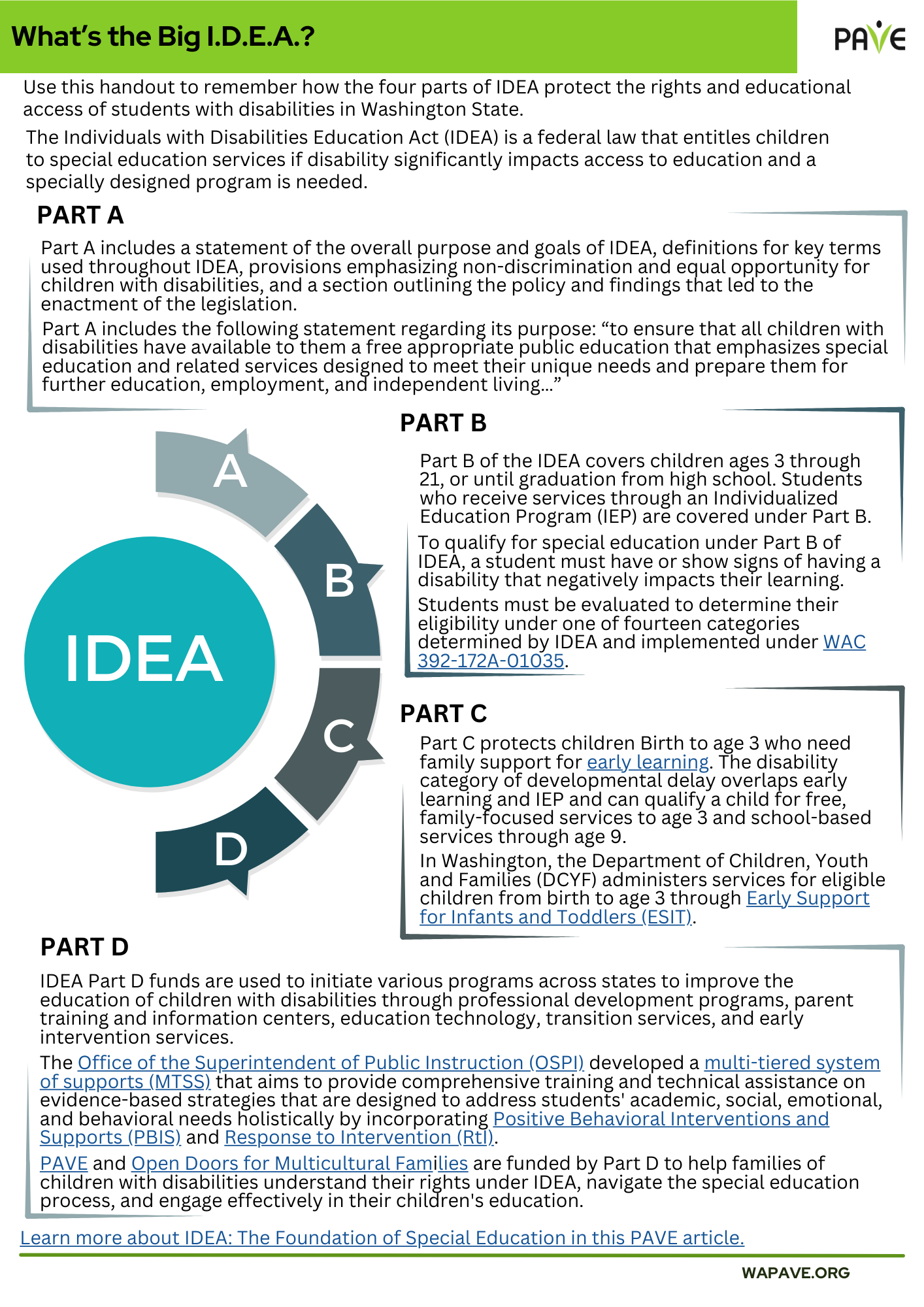
- School districts are responsible for searching for, finding and evaluating (testing) all students who show signs of having disabilities that affect their education. This includes students who are home schooled or placed in private schools by their parents, under the Child Find section of the Individuals with Disabilities Education Act (IDEA). The evaluation shows whether a student is eligible for special education and related services.
- Public school districts must re-evaluate students who are eligible for special education at least every three years and include them in their records, even if those students attend private schools.
- When a family chooses to enroll their student with disabilities in a private school, they have different rights than if their student was in a public school.
- Public school districts may offer limited support through a services plan, which is developed together with families and private schools.
- Available services vary by district and may include specialized instruction (special education) or related services, but not all a student’s needs may be met.
- Parents have an important part in helping teachers and school staff decide which available services and supports will be used for their child. When parents go to meetings and talk with teachers and school staff they can help create a services plan to help their child learn in school and join school activities.
Child Find and Special Education in Public and Private schools
All students have the right to be evaluated (tested) for special education if there is reason to believe a disability may affect their learning, whether they attend public or private schools. This protection is from Child Find, a part of the Individuals with Disabilities Education Act (IDEA). It requires public school districts to find and test students with possible disabilities.
An evaluation shows if a student is eligible for special education services because of a disability that affects the student’s ability to learn from a school’s general education program to the point where individualized instruction and support is needed. Once a student is found eligible for special education, the next step depends on their school placement, private or public school. A student may begin in a public school and change to a private school or begin at a private school and then change to a public school.
It’s possible that students with disabilities in private schools may not receive any special education services. One reason might be that their family doesn’t want them. In those situations, the local public district is still responsible for keeping track of that student and including them in their records. The district is also responsible for re-evaluating those students for eligibility at least every 3 years.
What should families know about private school placement?
Choosing a private school for a child with disabilities can be a thoughtful and hopeful decision, offering new opportunities and environments that may better suit a child’s needs. It also raises important questions about legal protections, available support, and what the public school district or the private school is responsible for in their child’s education. Understanding these differences is key to making informed decisions and ensuring that a child’s school experience is as inclusive and supportive as possible.
When families choose to enroll their child in a private school based on personal preference, this is called “parental placement” or “parentally placed” under IDEA and implemented under Washington Administrative Code (WAC 392-172A-04035). These students keep some protections under federal law, though they are different from the protections in public schools.
There are two types of placement which have different results for getting special education services:
Placement by a student’s IEP team
Students in public schools using special education might be placed in private schools by [their IEP team] so they can get the Free Appropriate Public Education (FAPE) that best suits their needs. Those students keep the full rights and protections of public school special education law
FAPE includes learning and other supports specifically chosen for a student with disabilities (individualized) to help them learn and make progress toward their goals. If a student is eligible based on evaluations (testing for disability that might affect learning), IDEA requires that the public school must provide FAPE and an Individualized Education Program (IEP).
Parental Placement based on a family’s personal choice
Parentally placed students in private schools are not entitled to FAPE or the full range of services available in public schools. Instead, they may be eligible for limited support funded by federal grants to states.
- Which supports and how much those supports depends on how much money is available. It also depends on which supports the community and public school district decide they want to spend the money on.
- Two disability rights laws still protect students in private schools: Section 504 of the Rehabilitation Act and the Americans with Disabilities Act (ADA). Under these laws, families may request accommodations and help plan supports so their child can access learning and participate in school activities.
What special education services can private school students get?
If a student going to or moving to private school qualifies for special education services, they do not receive an IEP. Instead, they may be served through a services plan, which outlines the supports they will receive.
The public school district, the private school, and the family together develop a services plan. It outlines the specific services a student will get and how they will get them. The public school district is responsible for checking on the services and the providers who deliver them.
Unlike an IEP, a services plan does not mean the parentally placed private school student must legally get those services, and it does not guarantee the same level or types of support.
Federal laws that apply to private schools and to a student’s services plan are
Federal law protects parents in their right to participate in the development of a services plan. According to federal guidance to states by the US Department of Education, (question E-3), “Given the emphasis on parent involvement in IDEA, the Department believes that parents should have the opportunity to participate in meetings to review and develop the services plan for their child.”
What types of services may be in the plan?
Services might include:
Special education services in a specific area of learning
Related services such as occupational, physical, or speech-language therapy
Adapted Physical Education
“Accommodations” based on Section 504 of the Rehabilitation Act (Section 504) and the Americans with Disabilities Act (ADA) , which apply in private schools.
- Section 504 is a federal law the prevents discrimination against individuals with disability, in all public and private places that are open to the public. This is why Section 504 applies to private schools. Students whose evaluation for Special Education showed they did not need an IEP but could still use help in school to be able to learn in class and participate in school activities can get supports through accommodations.
- ADA is a federal law that also prevents discrimination against individuals with disabilities and makes sure individuals with disabilities have the chance to learn and participate at school.
Some types of accommodations are:
- Longer time periods to finish homework and take tests
- Use a different way to learn, like listening to an audiobook instead of reading one
- Record a lesson instead of taking notes
- Use a calculator
- Giving a student a different way to show they have learned something
- Using Assistive Technology [LINK]
- Use a quiet area to learn or take tests
- Use a sensory device, like a fidget device or chair band
Accommodations can also be designed for other situations, based on what a student needs. They can be very flexible and useful in a services plan.
Where do services in the services plan take place?
Services for students with disabilities in private schools can be given in a variety of places. These may be the private school itself, a public school, or another place that parents agree to in the services plan. In most cases, transportation to get to services is the responsibility of the public school district.
The U.S. Department of Education recommends that services be provided on-site at the child’s private school whenever possible to minimize disruption to the student’s educational experience.
NOTE: The public school district responsible for providing them is the one where the private school is located—not necessarily the district where the student lives. This applies even if the student attends school in another county, state, or country.
How do they decide which services and supports will be offered by private schools?
In Washington State, each spring, public school districts meet with private schools and community members to plan how to support students with disabilities. This process is called consultation. It helps decide what services will be offered through federal programs, even if those services are different from what public school students receive.
The consultation decides:
- Which services will be offered.
- How services will be provided.
- How success will be measured.
Consultation keeps going during the year and includes opportunities for private schools and families to share their thoughts. Parents are encouraged to ask how their school or district participates in this process and what services are being decided on.
Because services are decided by local priorities, not all student needs may be met. For example, a district may choose to offer speech/language services but not occupational therapy.
Once services begin–usually in early fall–the public school district works with the private school to make sure everything is running smoothly. They check in regularly to see if the services are helping students and make changes if needed.
Private schools share data like test scores or language assessments (tests) to help guide the process. Together, the district, school, and service providers look at how well the services are working and decide if anything needs to be adjusted.
How are services for private school students funded?
Federal law requires public school districts to use some of their federal IDEA Part B funds to support students with disabilities enrolled in private schools by their families. This amount is calculated with a formula called proportionate share, based on the number of eligible students attending private schools. Families can ask for specific details about the local requirements for proportionate share by going to the district’s annual consultation.
What can parents do if they disagree with educational decisions about their child’s evaluations or services?
Dispute resolution is a process used under IDEA to help parents and schools fix disagreements about a student’s need for special education, what is in a student’s IEP, and how well the school is doing providing the learning and services in the IEP. The Center for Appropriate Dispute Resolution in Special Education (CADRE) provides parent guides and videos explaining the dispute resolution options.
Parents have the right to request an Independent Educational Evaluation (IEE) at public school district expense if they disagree with an evaluation conducted by the public district (WAC 392-172A-05005). PAVE provides a sample letter to request an IEE in the article: Evaluations Part 2: Next Steps if the School Says ‘No.’
If families have concerns about how services are provided, or feel the consultation process was unfair or their input wasn’t considered, they can take the following steps:
- Start by contacting the public school district to discuss the concern.
- If unresolved, the Disagreements and Complaints page at the Office of the Superintendent of Public Instruction (OSPI), WA State’s Education Department, will show you your choices for action and gives contact information.
- If necessary, file a formal Community Complaint with OSPI.
- These steps are in place to make sure families and schools have a voice and can advocate for the services their students need.
Other dispute resolution options are limited when a student is in private school. For example:
- Due Process hearings are only available for complaints related to Child Find.
- Mediation is offered only for complaints related to Child Find or Community Complaint issues.
- Families cannot demand compensatory services if the district has run out of its proportionate share funds. Compensatory services are additional services provided when a student was available to receive services as written by a program or plan; however, the school failed to provide them.
What should families keep in mind?
Students in public schools who qualify for special education receive an IEP and are entitled to FAPE. This includes individualized instruction and supports designed to help them make progress toward their goals.
Students in private schools do not receive FAPE and are not entitled to the same level of services. Instead, they may receive limited support through a services plan developed by the public school district together with the private school and the parents. These services are based on available funding and local priorities.
Families should keep in mind:
- Accommodations under Section 504 and the ADA still apply in private schools.
- Public school districts are responsible for evaluating students and keeping track of eligibility for special education.
- Service plans in private schools are not guaranteed to meet all needs and do not include direct funding or reimbursements.
- The consultation process decides which services are offered and how they are delivered.
- Parents have the right to participate in planning and to decide to use dispute resolution if concerns arise.
Families can advocate (stand up) for their child’s needs in a private school by staying informed, asking questions, and participating in consultation. With the right information and active involvement, families can help create a learning experience that supports their child’s growth and success—no matter what type of school they go to!
Learn More
- Child Find: Schools Have a Legal Duty to Evaluate Children Impacted by Disability
- IDEA: The Foundation of Special Education
- Evaluations Part 1: Where to Start When a Student Needs Special Help at School
- Section 504: A Plan for Equity, Access and Accommodations
- Transitioning Rights and Accommodations from IDEA to ADA and 504
- FAPE Fits Like a Proper Outfit
- Steps to Read, Understand, and Develop an Initial IEP
- Evaluations Part 2: Next Steps if the School Says ‘No.’
- When Parents and Schools Disagree: Navigating Special Education Disputes