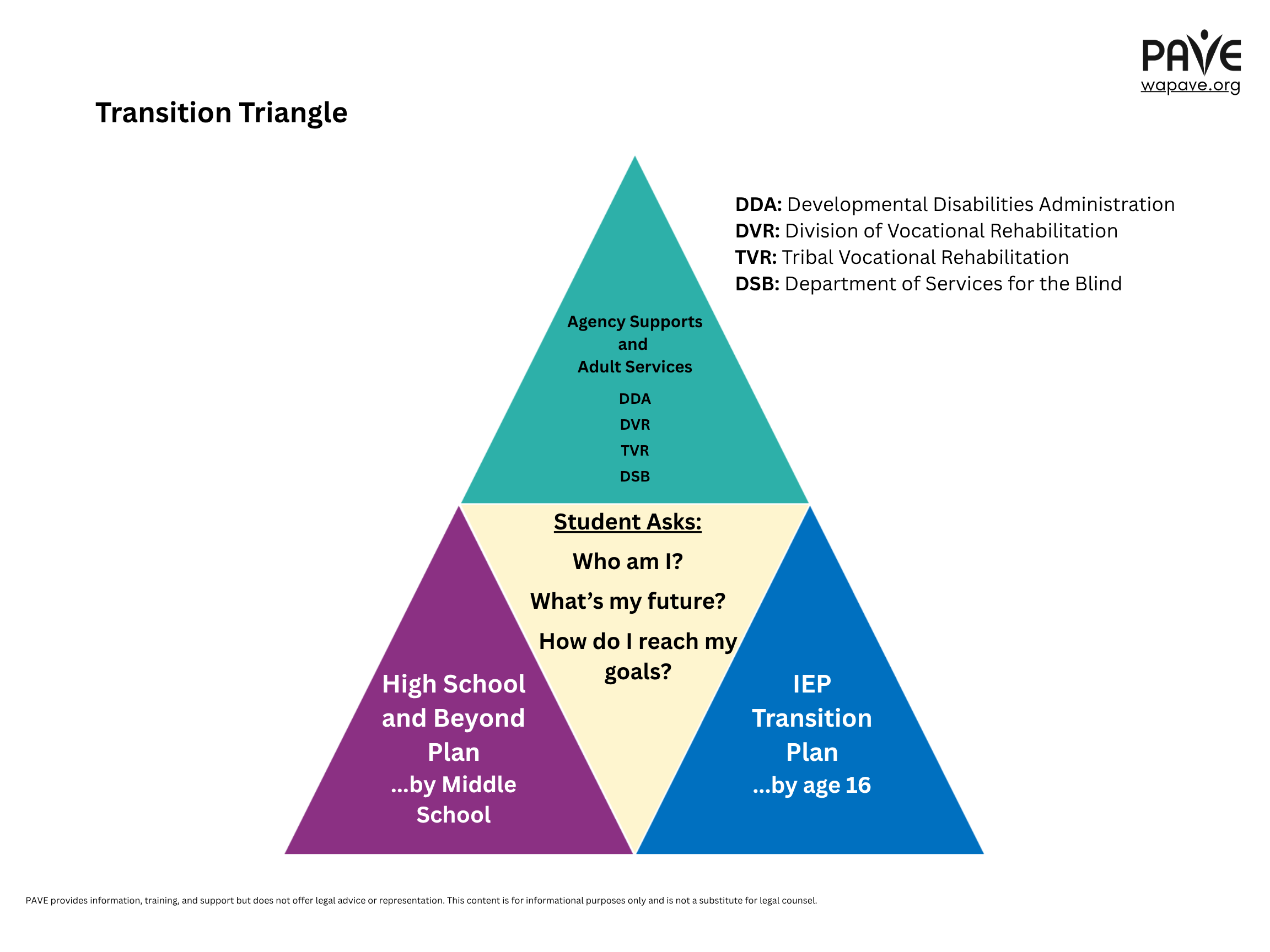
Helping a student with disabilities prepare for Life After High School requires thoughtful organization and planning. This presentation describes three ways to support this important time of life. This triangle shows the three tools we’re going to talk about.
Helping a student with disabilities prepare for life after high school requires thoughtful organization and planning. This presentation describes three ways to support this important time of life. This triangle shows the three tools we’re going to talk about. Notice that the center of the triangle includes three questions for a young person to consider: who am I, what’s my future, and how do I reach my goals? The three colored triangles show different ways that adults can help a student ask and answer those questions. We’re going to talk about all three tools in this training. Let’s start with the purple triangle on the bottom left corner. This tool is called high school and beyond plan. Schools in Washington state are required to help students start high school and beyond plan before they leave middle school. The school’s counseling staff is usually responsible to support each student in building a high school and beyond plan. Think of the high school and beyond plan as a personalized pathway through school. This tool is provided for all students, not just students with disabilities. By the end of 8th grade, a student has completed a career interest and skills inventory to consider education and career goals. That’s part of the plan. The student might be considering going to a university or a technical college. They might want to do an apprenticeship program or get an industry standard certificate to do a specific job. Maybe they’re thinking about military training, on the job training, or something else. All are considered as part of high school and beyond planning. Thinking about the future helps with decisions about what to focus on now. Of course, most students change their plans many times.
That’s why the high school and beyond plan is reviewed at least once a year. Keep in mind that the students vision for their future is the focus of the plan. These are the three questions every high school and beyond plan is required to address: who am I, what can I become, how do I become that? You might notice these questions match the questions in the center of our transition triangle. This is where the whole process begins, with these questions. It’s never too early to start talking to a student about these questions. Discussing these questions with many different people in many different settings is part of high school and beyond planning. This is not a single interview. It’s a long-term discussion that happens while a student is moving through school and toward graduation. If the high school and beyond plan is a new concept for you, take a moment to pause and consider who at your school might provide more information about this process.
Perhaps take a moment to write yourself a reminder note to get more information. Could you contact your students counselor, the IEP case manager, a school administrator, or maybe a favorite teacher? Could you ask your student? The state instructs schools to include family caregivers in this process. Remember that a completed high school and beyond plan is required for a student to graduate from a high school in Washington state. Let’s look at the blue triangle on the lower right side of our transition triangle so we can talk about the IEP transition plan. The individualized education program, IEP, is required to include a transition plan by the school year when a student turns 16. This plan is an IEP team project.
Keep in mind that the student and parents are important members of the IEP team. Here’s some information to better understand this required part of a student’s school services program. The federal law that governs special education is the Ida, which stands for individuals with disabilities education act. Laws about IEP process are mostly from idea part B. Part A is also important when we’re talking about adult life planning. Part A of the idea describes the laws purpose. The statement on this slide is from idea part A. It says that special education is provided to ensure that all children with disabilities have available to them a free and appropriate public education designed to meet their individual needs and prepare them for further education, employment, and independent living. In simpler words, supporting students with disabilities to make a smooth transition into adult life is part of a school’s basic responsibility.
Here’s some information about the IEP transition plan. Most importantly, the plan is built from the students needs, preferences, interests, and strengths. Once the plan is written into the IEP, it drives the program. The annual goals all connect in some way to the students adult life plan. The IEP transition plan includes adult living objectives in three areas: postsecondary education, acquisition of daily living skills, and vocational evaluation and support. Washington schools receive guidance from the office of superintendent of public instruction, OS Pi, our state educational agency. OSPI provides model forms to support schools and families when developing an IEP. This form shows what to include in an IEP when transition programming is added.
This section of the model form shows that a student must be invited to IEP meetings once transition planning is included, and an age appropriate transition assessment is required. Transition assessments include a range of tools, including surveys and questionnaires, profiles and portfolios, vocational assessments, interviews, and more. This form makes clear that a transition plan is not built from a quick meeting but is a multi-part process. State guidance is clear that the IEP transition plan is intended to support rather than replace the students high school and beyond plan. Here’s some questions you can consider to make sure the transition plan is well written: is the plan age appropriate? Goals should be achievable but not too easy, based on the age and abilities of the student. Is information provided by more than one source? This is a long-term project with many participants. Is a target graduation date included? The IEP team decides when a student will graduate, and the family is part of that decision process. Are the annual goals relevant to the long-term goals? Do the postsecondary goals consider all areas of life after high school? And keep this one in mind: does the IEP align with the students high school and beyond plan? The state educational agency ospi provides information about how the high school and beyond plan and the IEP transition plan are supposed to work together.
Here’s a visual list of the four areas to cover in transition planning: employment, further education, independent living, and community engagement. Remember the three questions for for our student. They are, who am I, what’s my future, and how do I reach the go my goals? Adults can help the student ask and answer those questions for each of these four areas of learning and life. Here’s something else to remember. The IEP ends when a student graduates from high school or ages out of services at 21. However, accommodations on the IEP can travel with the student into higher education, vocational programming, or work. The accommodations are protected by federal civil rights laws, including Section 504 of the Rehabilitation Act. Those protections are for the lifespan. High school is a great time to make sure accommodations are individualized and well written, and that the student knows what they are and how to ask for them.
Let’s look at the last part of our transition triangle. The teal triangle at the top represents public agencies that might support a young person to get a job. I will explain what each of these means in a few moments. All these agencies provide individualized support that may help a young person get ready for work, get a job, or keep a job. Eligibility criteria IA for each of these agencies is a little bit different, and you must apply to access their services. Some agencies offer programs to help students with disabilities explore work and self advocacy while they are still in school. Those services are called pre-employment transition services. Pre-employment transition services might include job EX exploration, work-based learning, counseling about higher education and how to gear up for college, workplace readiness, and self-advocacy, like special education rights. Vocational rehabilitation rights are protected by law.
If these service agencies are new to you, consider if you want to get more information about how to involve an outside public agency in life after high school planning. Maybe a school counselor, administrator, or teacher could help, or maybe it’s a question for your IEP team. Sometimes special education district staff can help contact these agencies with you. Staff at pave can also help you research your options. Click get help at our website wapave.org to request our support. So take a moment, if you want to write down an idea so you remember to follow up. I’m going to tell you more about each of these agencies on the next
slide. You may want to reach out directly to one of these agencies by looking them up online. DDA is the developmental disabilities administration. DVR is the division of vocational rehabilitation. TVR is tribal vocational rehabilitation for Native Americans with disabilities. dsb is the department of services for the blind, for people with blindness or low vision. The next few slides have additional information to help with your students life after high school planning. Everyone in the family needs to keep in mind that when a student turns 18 in Washington, they are responsible for their own educational decisions. If the student is ready and able to take charge, nothing needs to happen. If the student still wants parents involved, then the student signs a letter of consent for parents to attend meetings and continue participating on the IEP team. Parents who have legal guardianship have a larger role in decision making and may not need their student to sign consent.
In Washington state, one legal option for supporting an adult with disabilities is called supported decision making. This slide shows an article available on PA’s website with more information about supported decision making and how to access a sample form. Families need to know that their students can participate in commencement and other senior year activities with their classmates even if they aren’t yet earning a diploma. That state right is protected by Kevin’s Law. School staff recommend that families plan early for senior year activities so appropriate accommodations can be provided. Listed on this slide are places that schools and families might get more help.
The three O’s are the Office of Superintendent of Public Instruction, the Office for Civil Rights, and the Governor’s Office of the Educational Ombuds. Another option is to reach out to one of the state’s nine educational service districts, the ESD’s. If the school district doesn’t have everything your student needs, you and the school might seek additional resources from the ESD that serves your area. Each ESD has a behavioral health navigator, for example, and some ESD’s are licensed to provide behavioral health services.
Another place to get help for supporting a loved one with a disability is the DD ombuds. This agency provides advocacy to support quality of life for people with developmental disabilities. Their staff can help individuals file complaints related to disability discrimination.
This training has been provided by parent training and information, PTI, a program of pave. We provide information, resources, and direct support. Click get help at wapave. org and one of our staff will contact you. You can also leave a message by phone to request help, and that number is 800 572 7368. If you need help with the accessibility of any of our resources, please let us know. We provide language translation options. Additional information on this topic is available as part of PAVE’s online toolkit called school to adulthood transition planning toolkit for high school life and work. Look for the button under the calendar on our website. Please note that pave is not a legal service organization and cannot give you legal advice or represent you. PTI’s funding comes from a US Department of Education grant, but the government doesn’t review our training materials in order to endorse them. We’d love to know whether this video was helpful for you. On the page where you found this video, there’s a link to a short survey. Thank you for sharing your feedback. Thank you for listening and learning, and please contact us if you need individualized assistance or further training opportunities.