
Simple instructions on how to find and use our toolkits!
Tag: special needs
I Have to Sign What? Healthcare in Transition
When young people turn 18, a lot happens. For instance, in Washington State, 18 is the age when a person legally becomes an adult and must handle tasks and make decisions that used to be made for them by adults.
Adult responsibilities and decisions can feel scary and confusing for the unprepared. Becoming responsible for medical care is part of growing up, and that process is so critical that there’s a specific name for it: healthcare transition.
For example, at age 18, a young adult is responsible for signing official paperwork to authorize procedures or therapies and to pay for co-pays. They must sign documents stating who can look at their medical records, speak with their doctors, or attend an appointment with them. Those rules are part of HIPAA, which stands for the Health Insurance Portability and Accountability Act. HIPAA is a federal law that protects confidentiality, regardless of disability. In this video, young adults living with various disabilities and medical conditions share their journeys through the adult healthcare system. They talk about how they make decisions and how they ask for help. Their ability to explain their needs, make decisions, and speak up for themselves is called self-advocacy. Take a look and listen to what they have to say in their own words!
Learning these skills isn’t something that happens the minute you turn 18. It takes practice to learn how to ask questions at the doctor’s office, to remember to ask about medications, to bring your insurance card. If you are a youth or young adult, those are things you can start early. If you are a caregiver or parent, begin giving your young adult or child questions to ask the doctor when they go in for well-child checks at age 12 or 13. Start talking with them about the conditions they may have and answer any questions they have honestly. If they are aware of why their body is doing what it is doing they can better manage their needs and ask for help when they need it. Help them learn to manage medicine with medicine reminder apps and pill containers. These kinds of things not only set them up for success when they are 18 at the doctor’s office, but also helps them advocate better for what they need in school and the community.
Here are some great sites that provide comprehensive step by step guidance to this process. See what fits best for yourself as a young adult; parents and guardians can think about what fits your family from their point of view.
- Got Transition has great tools and videos for youth, families, and providers. Young adults and families developed it, so it is peer-based.
- Charting the LifeCourse™ was created by families to help individuals and families of all abilities and all ages develop a vision for a good life, including their health care.
- The Center for Transition to Adult Health Care for Youth with Disabilities is a national health care transition resource center. The goal of the center is to empower youth and young adults with intellectual and developmental disabilities (ID/DD), ages 12-26, to direct their own transition from pediatric to adult care, with no reduction in quality of care and no gaps in services.
Including Healthcare Needs and Goals in the Transition Plan
Healthcare transition is often left out of the transition process and left to parents and students to do themselves. Parents, students, and everyone on the IEP team should think about how health and healthcare can affect a student’s goals for college, work, and living on their own. Parents and students can ask that this be a part of the transition plan and can use the resources listed above in the planning process.

Insurance in Healthcare Transition
Healthcare transition, like all other aspects of transitioning to adult community living, employment, and services, can be difficult. However, if teenagers and families plan ahead for the healthcare changes that occur when a child becomes an adult, things can go more smoothly and successfully. Here are some resources and information to help make the transition to adult care effectively and give young adults more confidence and self-assurance.
There are two main components for individuals transitioning from pediatric (children) to adult health care:
- New medical providers and systems, including changes in insurance
- The young adult’s new responsibility of being in charge of their own health care
Health Insurance and Providers
Whether an individual is on Medicaid, Medicare, or private health insurance, eligibility, costs, and covered services may change.
Washington’s Medicaid option, Apple Health, has different financial requirements for adults than it does for minors. The type of Medicaid a youth has before age 18 may change depending on the source of their income or benefits when they turn 18.
If the disability is significant, a student or young person may be on classic Medicaid. When they turn 18, they must contact the managed care organization (MCO) that is their current healthcare provider (Molina, Community Healthcare, Well Point, etc.) and:
- Confirm who their current healthcare provider is
- Confirm their own current address
They must do this every 12 months.
If the youth is not
- on Supplemental Security Income (SSI),
- receiving Developmental Disability (DDA/DDCS) services,
- or receiving state benefits for the blind such as Aging, Blind, or Disabled (ABD) Cash Assistance or State Supplementary Payment (SSP),
then they may be on Medicaid through the healthcare exchange, the Washington Health Plan Finder.
At 18, Washington youth are required to apply for or renew Apple Health by going to the Health Plan Finder website. Even if an individual is not eligible for fully subsidized (paid) healthcare, the Health Plan Finder can reveal some low-priced options.
Young adults who are on their parents’ private insurance will be covered under their parents’ plan until they are 26, unless the young adult works and are covered through an employer-based plan. When they turn 26, if they are not working and are not covered by SSI/SSDI, DDA/DDCS services, or any other disability based supports, they will need to apply for their own health insurance. Again, the Health Plan Finder can help you find affordable options, including Apple Health.
For individuals under 65 who are receiving Medicare due to a disability, insurance should not change due to the transition to adulthood. It is important to know which doctors can treat an individual’s conditions and whether an insurance plan includes those doctors. To find out, call the MCO/health provider’s helpline or view their website to find out whether those doctors are included in their insurance plan. The doctor’s office will also give information on which plans they accept and which ones they don’t.
Taking on Responsibility for Health Care and Decisions
Healthcare is just one of many new responsibilities that young people take on as they become adults. Parents can avoid overwhelming a teen with new obligations, by beginning with giving younger teens options and increasing tasks to help them adapt to this change. There are several resources for families and youth to use in this transition:
- Family to Family has a youth-written curriculum about Transitioning to Adult Doctors to help teens start their medical transition journeys.
- Charting the LifeCourse™ was created by families to help individuals and families of all abilities and all ages develop a vision for a good life, including their health care.
- Got Transition is a comprehensive website about the transition to adult health care, with quizzes, FAQs, and timelines to make it easier to understand.
- The Center for Transition to Adult Health Care for Youth with Disabilities is a national health care transition resource center. The goal of the center is to empower youth and young adults with intellectual and developmental disabilities (ID/DD) ages 12-26 to direct their own transition from pediatric to adult care with no reduction in quality of care and no gaps in service.
Beyond these resources, the most useful resource are young adults themselves. Whether you are a parent/caregiver or a transitioning individual, it’s important to recognize that lived experience provides knowledge, even in a new situation. Parents, caregivers, and young adults have knowledge of medical needs that may not be in a chart. They know about the emotional or behavioral challenges a young person has. They know the youths’ strengths, areas for growth, other important things only an individual and their family know.
Write out what you feel is most important in your health care journey over the next 5 years. What do you need to know from doctors? What do you need to know about school and work? What do you need to know about your condition? Be curious and remember what you have already done to take care of yourself. Ask your parents and caregivers about what they see as important over the next few years. Take the time to explore, then start the transition journey to adult care with an idea of what you would like.
Another group to consult are your current medical providers and specialists. They have helped many other teens transition to adult healthcare, and they are a part of developing the care plan, a critical resource for transitioning to an unfamiliar doctor or clinic when a young adult may have complex care needs. Doctors’ office staff are also used to dealing with these issues and may have some good planning advice for families. Lastly, advice from families who have already helped a child transition to adult care can know what to do and what not to do! Parent-to-Parent can match parents up with families who have already gone through such transitions with those who seek their knowledge and experience. Informing Families has some good basic resources on its website for getting started.
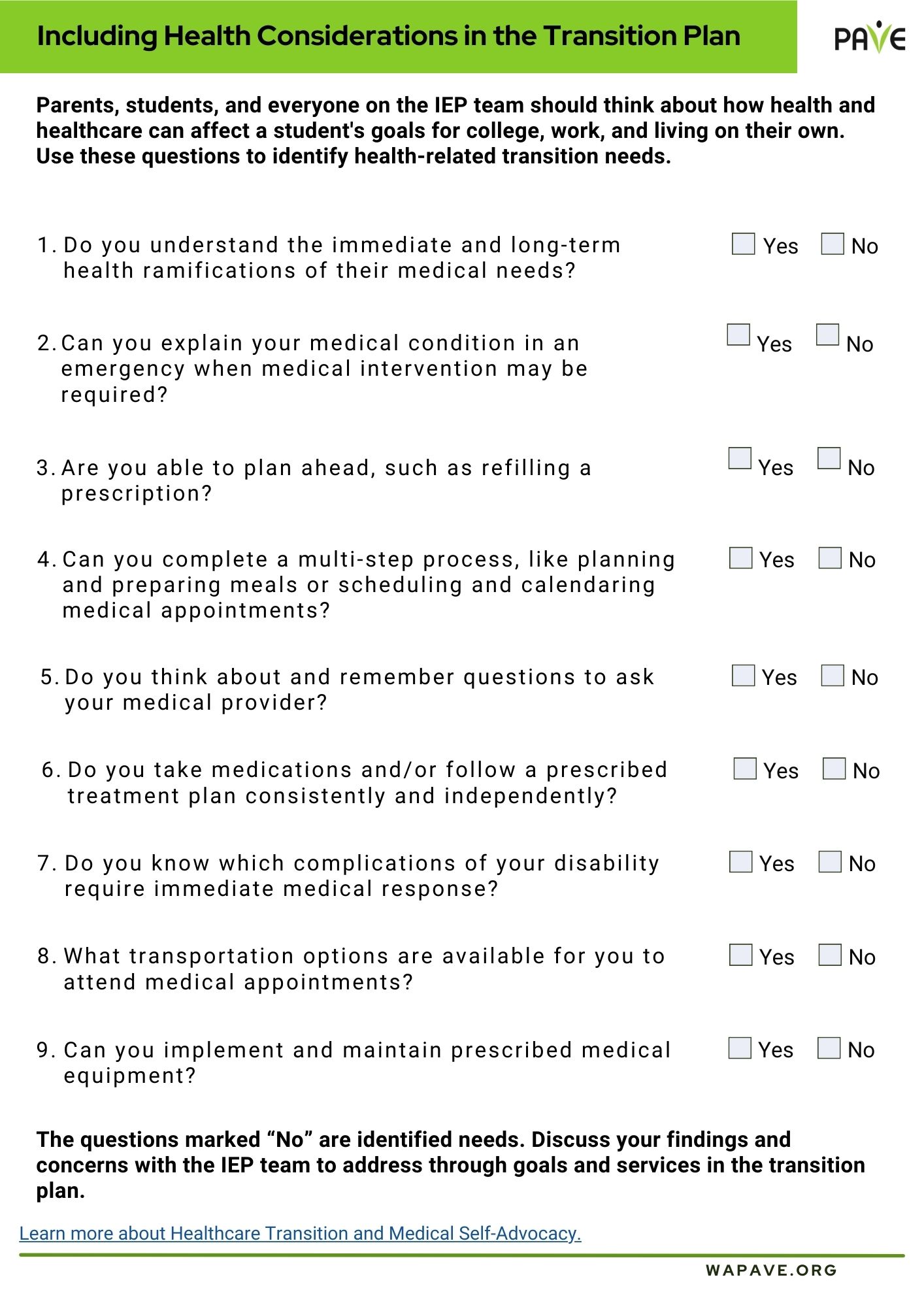
Including Health Considerations in the Transition Plan
Parents, Students, and everyone on the IEP team should think about how health and healthcare can affect a student’s goals for college, work and living on their own. PAVE has made a fillable form that you can download when starting to think about this area in transition.
Download the document Including Health Considerations in the Transition Plan
Self-Care is Critical for Caregivers with Unique Challenges
Caring for individuals with disabilities or complex medical needs can be emotionally and physically draining, making intentional self-care essential for long-term well-being. Simple practices like mindfulness, getting enough sleep, going for a walk, or taking a few deep breaths can help reduce stress and build resilience. Talking to others who understand and finding time to rest can also help caregivers stay strong and healthy.
A Brief Overview
- Self-care is not selfish. Self-care is any activity or strategy that helps you survive and thrive in your life. Without regular self-care, it can become impossible to keep up with work, support and care for others, and manage daily activities.
- PAVE knows that self-care can be particularly challenging for family members caring for someone with a disability or complex medical condition. This article includes tips and guidance especially for you.
- PAVE provides a library with more strategies to cultivate resilience, create calm through organization, improve sleep, and more: Self-Care Videos for Families Series.
Introduction
Raising children requires patience, creativity, problem-solving skills and infinite energy. Think about that last word—energy. A car doesn’t keep going if it runs out of gas, right? The same is true for parents and other caregivers. If we don’t refill our tanks regularly we cannot keep going. We humans refuel with self-care, which is a broad term to describe any activity or strategy that gives us a boost.
Self-care is not selfish! Without ways to refresh, we cannot maintain our jobs, manage our homes, or take care of people who need us to keep showing up. Because the demands of caring for someone with a disability or complex medical condition can require even more energy, refueling through self-care is especially critical for caregivers.
Two Feet, One Breath
Before you read anymore, try this simple self-care tool called Two Feet, One Breath. Doctors use this one in between seeing patients.
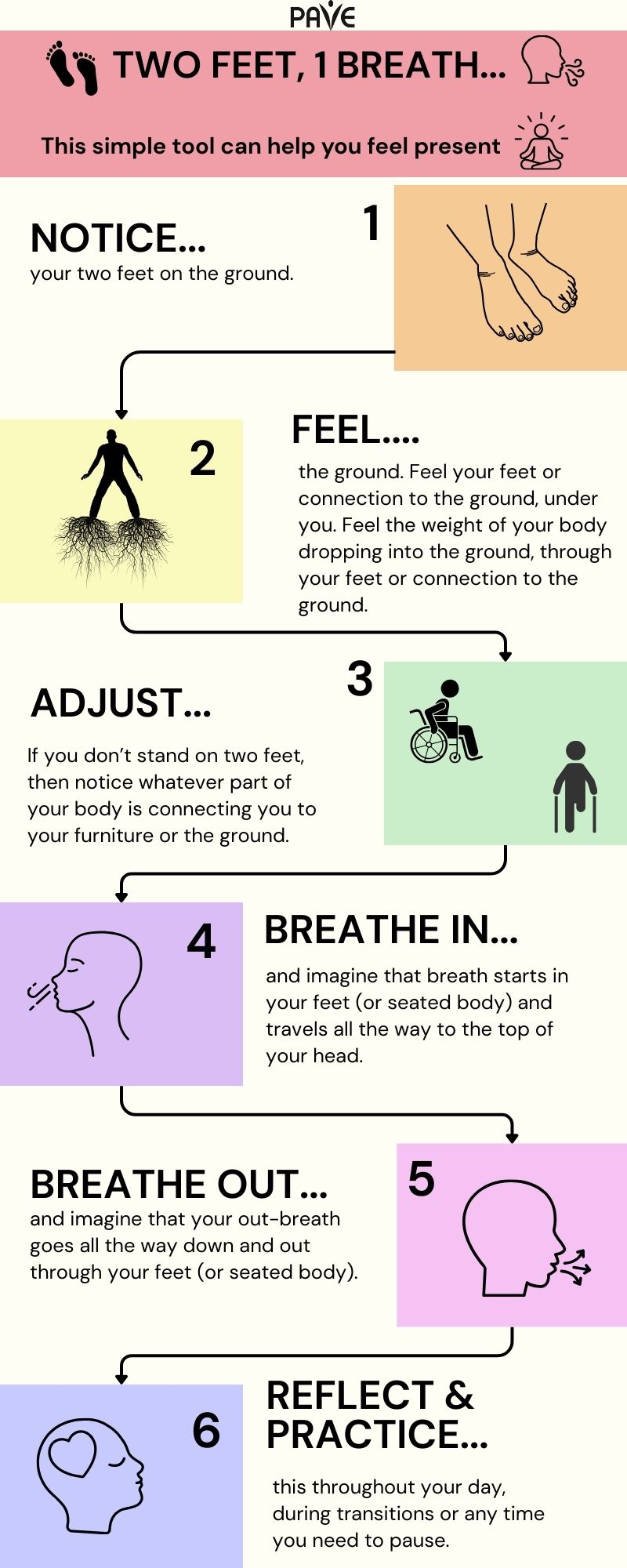
Download this infographic, Two Feet 1 Breath:
English | Chinese (Simplified) 中文 (Zhōngwén) | Korean 한국어 (Hangugeo) | Russian Русский (Russkiy) | Spanish Español | Tagalog | Vietnamese Tiếng Việt
Two Feet, One Breath can become part of every transition in your day: when you get out of bed or the car, before you start a task, after you finish something, or any time you go into a different space or prepare to talk with someone. This simple practice highlights how self-care can become integrated into your day.
Although a day at the spa might be an excellent idea, self-care doesn’t have to be fancy or expensive to have a big impact!
Almost everyone knows or cares for someone with special needs. According to the Centers for Disease Control (CDC), at least 28% of the American population experiences a disability. The result is widespread compassion fatigue, which is a way to talk about burnout from giving more than you get.
Below are some ways to use self-care to avoid burnout!
Connect with others
Building a support network with others who share similar life experiences can be incredibly valuable. When you’re going through a challenging or unique situation—like parenting a child with special needs or managing a family health issue—it can feel isolating. These connections offer emotional validation and a sense of understanding that can be hard to find elsewhere—you don’t have to explain everything because others simply get it. Research shows that social support can significantly reduce stress, anxiety, and depression, enhancing overall well-being and resilience. Beyond emotional comfort, support networks empower individuals by helping them build confidence, understand their rights, and even engage in advocacy efforts that benefit their families and communities.
Here are some communities and resources to help you get connected:
Parent-to-Parent Connections
The Parent-to-Parent network can help by matching parents with similar interests or by providing regular events and group meetings.
Support for Families of Youth Who Are Blind or Low Vision
Washington State Department of Services for the Blind (DSB) offers resources and support for families. You can also hear directly from youth about their experiences in the PAVE story: My story: The Benefits of Working with Agencies like the Washington State Department of Services for the Blind.
Support for Families of Youth Who Are Deaf or Hard of Hearing
Washington Hands and Voices offers opportunities for caregivers of youth who are Deaf or Hard of Hearing (DHH) to connect, share experiences, and find community.
Resources for Families Navigating Behavioral Health Challenges
Several family-serving organizations provide support, education, and advocacy for caregivers of children and youth with behavioral health conditions:
- Family, Youth, and System Partner Round Table (FYSPRT). Regional groups are a hub for family networking and emotional support. Some have groups for young people.
- Washington State Community Connectors (WSCC). WSCC sponsors an annual family training weekend, manages a Substance Use Disorder (SUD) Family Navigator training, and offers ways for families to share their experiences and support one another.
- COPE (Center of Parent Excellence) offers support group meetings and direct help from lead parent support specialists as part of a statewide program called A Common Voice.
- Dads Move works to strengthen the father’s role in raising children with behavioral health needs through education, peer support and advocacy.
- Healthy Minds Healthy Futures is an informal network on Facebook.
PAVE provides a comprehensive toolkit for families navigating behavioral health systems, including guidance on crisis response, medical care, education, and family support networks.
Get Enough Sleep
The body uses sleep to recover, heal, and process stress. If anxiety or intrusive thinking consistently interrupts sleep, self-care starts with some sleeping preparations:
- Turn off screens after 7 pm, or use a blue-light filter
- Pre-load sleepy music or a calming meditation onto your phone or tablet
- Finish the evening with an herbal tea, such as chamomile
- Check out PAVE’s video: Body Sensing Meditation for Help with Sleep
- For more ideas, visit SleepFoundation.org
Move Your Body
Moving releases feel-good chemicals into the body, improves mood, and reduces the body’s stress response. Walk or hike, practice yoga, swim, wrestle with the kids, chop wood, work in the yard, or start a spontaneous living-room dance party.
The Mayo Clinic has this to say about exercise:
- It pumps up endorphins. Physical activity may help bump up the production of your brain’s feel-good neurotransmitters, called endorphins. Although this function is often referred to as a runner’s high, any aerobic activity, such as a rousing game of tennis or a nature hike, can contribute to this same feeling.
- It reduces the negative effects of stress. Exercise can provide stress relief for your body while imitating effects of stress, such as the flight or fight response, and helping your body and its systems practice working together through those effects. This can also lead to positive effects in your body—including your cardiovascular, digestive and immune systems—by helping protect your body from harmful effects of stress.
- It’s meditation in motion. After a fast-paced game of racquetball, a long walk or run, or several laps in the pool, you may often find that you’ve forgotten the day’s irritations and concentrated only on your body’s movements. Exercise can also improve your sleep, which is often disrupted by stress, depression and anxiety.
Be Mindful
Mindfulness can be as simple as the Two Feet, One Breath practice described at the top of this article. Mindfulness means paying attention or putting your full attention into something. Focusing the mind can be fun and simple and doesn’t have to be quiet, but it should be something that you find at least somewhat enjoyable that requires some concentration. Some possibilities are working on artwork, cleaning the house or car, crafting, working on a puzzle, cooking or baking, taking a nature walk, or building something.
For more mindfulness ideas, check out PAVE’s Mindfulness Video Series. From this playlist, Get Calm by Getting Organized, explores how getting organized provides satisfaction that releases happiness chemicals and hormones.
Schedule Time
A day can disappear into unscheduled chaos without some intentional planning. A carefully organized calendar, with realistic boundaries, can help make sure there’s breathing room.
Set personal appointments on the calendar for fun activities, dates with kids, healthcare routines, and personal “me time.” If the calendar is full, be courageous about saying no and setting boundaries. If someone needs your help, find a day and time where you might be able to say yes without compromising your self-care. Remember that self-care is how you refuel; schedule it so you won’t run out of gas!
Time management is a key part of stress management! This article, “Stress Management: Managing Your Time” from Kaiser Permanente, gives tips for managing your time well, so you can reduce the pressure of last-minute tasks and make space for the things that matter most to you.
Seek Temporary Relief
Respite care provides temporary relief for a primary caregiver. In Washington State, a resource to find respite providers is Lifespan Respite. PAVE provides an article with more information: Respite Offers a Break for Caregivers and Those They Support.
Parents and caregivers of children with developmental disabilities can seek in-home personal care services and request a waiver for respite care from the Developmental Disabilities Administration (DDA). PAVE provides two training videos about eligibility and assessments for DDA. For more information about the application process, Informing Families provides a detailed article and video.
Download the Emotional Wellness Tips for Caregivers
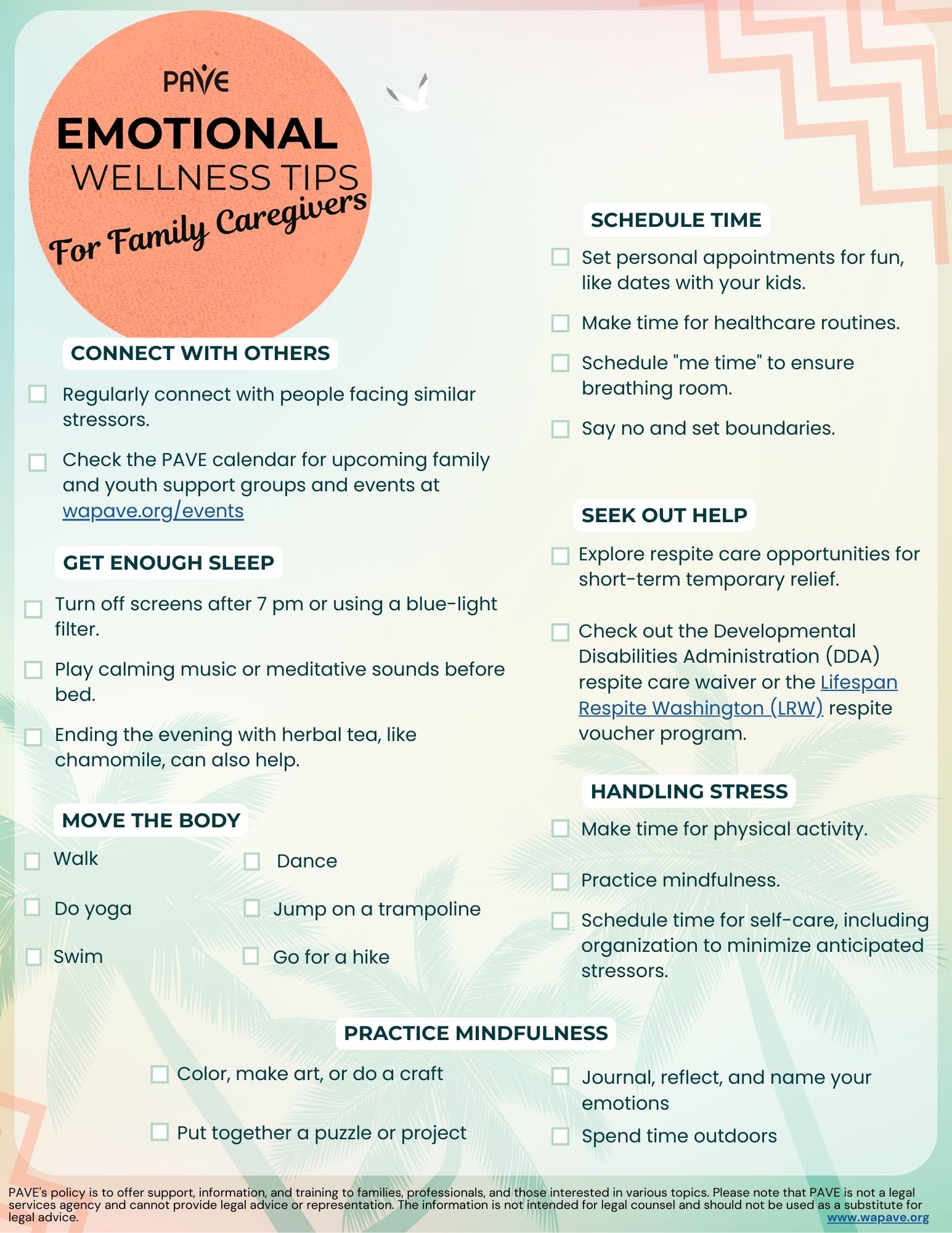
Download this checklist of Emotional Wellness Tips for Caregivers in:
English | Chinese (Simplified) 中文 (Zhōngwén) | Korean 한국어 (Hangugeo) | Russian Русский (Russkiy) | Somali Soomaali | Spanish Español | Tagalog | Vietnamese Tiếng Việt
Childcare-What to Know When Your Child has a Disability
When a parent or family caregiver needs care for their child with a disability, finding safe, appropriate, and affordable care will be a priority. There are resources for children with disabilities and their families in Washington State to find safe and affordable childcare. For providers which take federal funds, civil rights laws protect access and appropriate services for children with disabilities and their families.
A Brief Overview
- Two reliable sites with lists of childcare providers in Washington State are WA State Department of Children, Youth, and Families at findchildcarewa.org, and Childcare Aware of Washington Family Center, which is also by phone at 1-800-446-1114.
- Childcare takes place in many different settings, licensed and unlicensed. A state license for childcare can help you decide if a childcare setting is safe. This article tells you how to find out if a provider is licensed.
- It’s good to ask certain questions before enrolling a child with a childcare provider. This article offers a sample list.
- Three laws protect the rights of children with disabilities in childcare settings that accept federal funding: Americans with Disabilities Act (ADA), Individuals with Disabilities Education Act (IDEA) Part C (Birth to Age 3) and Part B (Age 3 through high school graduation) and Section 504 of the Rehabilitation Act of 1972.
- Childcare can be expensive. This article explains about tax credits and state programs that help working families, free early learning programs and preschool, and financial help when family, friends, or neighbors provide childcare for your child.
How can I find listings for childcare in WA State?
Use this link for listings on the Washington State Department of Children, Youth, and Families (DCYF): findchildcarewa.org
Washington State partners with Child Care Aware of Washington Family Center. The phone number for individual assistance with your childcare search is 1-800-446-1114
How can I find out if a childcare center, program, or family home childcare is safe?
By law, Washington State licenses certain childcare settings. Licensing sets standards that childcare programs and providers must meet. State inspections help ensure that licensed programs and providers meet the standards, which cover a wide range of topics, from the safety and cleanliness of the physical setting through number of staff per child, staff training, and age-and-ability appropriateness of activities and education.
Links to Washington’s licensing rules are on DCYF’s page on Becoming a Licensed Child Care and Early Learning Provider.
Licenses are required for:
- Family home early learning programs:
An early learning program licensed by the department where a family home licensee provides childcare or education services for 12 or fewer children in the family living quarters where the licensee lives. - Childcare center early learning programs:
A facility providing regularly scheduled care for a group of children aged from birth through 12-years-old for periods of less than 24 hours a day. - School-age programs (might provide before and after-school childcare and school vacation care):
A facility providing regularly scheduled care for a group of children 5 through 12-years-old for periods less than 24 hours a day, when children are not attending school. - Outdoor Nature-Based program:
An early learning program that offers regularly scheduled care for preschool-age children, school-age children, or mixed-age children for periods less than 24 hours a day, when children are not attending school.
What types of childcare don’t need a license?
- A nanny or babysitter in your family’s home
- Informal parent cooperatives (example: “babysitting exchange”)
- Play groups
- Educational preschools that operate less than four hours a day
- Parks and Recreation programs run by cities and towns
- Family members, friends, and neighbors who provide occasional care (If friends or neighbors are providing childcare for multiple children on a regular basis, they are required to have a state license.)
Programs operated by cities and towns may have standards set by the local government. Contact your local Parks and Recreation Departments to find out what standards their facilities need to meet, how staff are chosen and background checked, and any other questions you have about whether a program will be safe and appropriate for your child.
Programs that operate on federal or state funding must meet Washington State licensing requirements, such as Head Start and Early Childhood Education and Assistance Program
(ECEAP).
More on Head Start and ECEAP under “How to pay for childcare.”
Find out if a program or provider is licensed by:
- Checking in-person to see if a license is posted
- Use “Child Care Check: an online search tool to get information about individual child care providers and early learning programs in Washington”
This search tool lets you search for licensing history (has the home or center ever lost its license?), state monitoring reports (did the inspectors find anything to worry about?) status of staff background checks (are they being done?) and more. The tool finds information in Washington State’s database of all licensed childcare facilities and home childcare providers.
Here is a downloadable, printable checklist of questions to ask when you visit a childcare setting. It’s from ChildCare Aware of Washington: Child Care Quality Checklist
Questions to ask a provider:
Questions to ask a provider when enrolling a child with disabilities into a childcare program. It’s important for parents to ask questions to ensure the provider can meet their child’s unique needs.
- What experience do you have caring for children with disabilities?
- Do you have staff trained in special education or disability support?
- What is your adult-to-child ratio, and how flexible is it for children needing more support?
- Are staff trained in administering medications or managing medical devices (e.g., feeding tubes, EpiPens, inhalers)?
- How do you support children with behavioral challenges?
- What is your approach to discipline, and how is it adapted for children with developmental or emotional disabilities?
- Can you create or follow an Individualized Care Plan or IEP?
- Are you willing to make reasonable modifications to activities, routines, or environments?
- Do you allow assistive technology or support items (e.g., communication devices, wheelchairs, noise-canceling headphones)?
Are there laws that support my child with disability and protect their rights in a childcare setting?
There are three laws that may apply to childcare settings:
- Americans with Disabilities Act (ADA)
- Individuals with Disabilities Education Act (IDEA), Part C (Birth to Age 3) and Part B (Age 3 through high school graduation)
- Section 504 of the Rehabilitation Act of 1972, usually referred to as “Section 504” or “504”
Title III of the Americans with Disabilities Act (ADA) applies to:
- Federal, state, and local government-agency programs. Examples of this are Head Start, ECEAP (preschools operated by local school districts), summer programs, and extended day school programs.
- Privately run childcare centers such as those licensed by Washington State. “Even small, home-based centers are covered by title III of ADA”
- Private childcare centers that operate on the property of a religious organization, leasing or renting space on that property.
ADA does NOT apply to childcare centers that are RUN by religious organizations, such as a church, temple, mosque, or synagogue.
ADA requires childcare providers to give both children and parents with disabilities an equal opportunity to participate in the provider’s programs and services.
- Centers cannot exclude children with disabilities from their programs unless their presence poses a direct threat to the health or safety of others or requires a fundamental alteration of the program.
- Centers must make reasonable modifications to their policies and practices to integrate children, parents, and guardians with disabilities into their programs unless doing so would constitute a fundamental alteration.
- Centers must provide appropriate auxiliary aids and services needed for effective communication with children or adults with disabilities, when doing so would not constitute an undue burden.
- Centers must generally make their facilities accessible to persons with disabilities. Existing facilities are subject to the readily achievable standard for barrier removal, while newly constructed facilities and any altered portions of existing facilities must be fully accessible.
This website has many examples of situations to help parents and childcare providers understand what the law requires: Commonly Asked Questions about Child Care Centers and the Americans with Disabilities Act.
Individuals with Disabilities Education Act (IDEA), Part C (Birth to Age 3):
Children aged birth to 3 who have a disability or are at risk for certain disabilities may be eligible for services under IDEA. For children who qualify, Part C of IDEA authorizes services to support and promote a child’s development “in their natural environment.” This usually means the family home and often, the child’s childcare setting.
Parents can request their child be evaluated (tested) to see if they are reaching expected developmental stages. If evaluators find that a child needs support, a Family Resource Coordinator (FRC) will help the family create an Individualized Family Services Plan (IFSP). Family members have important roles in that plan, and professional staff provide services and help the family to use natural learning opportunities like playtime, meals, or baths to create opportunities for a child to practice and develop delayed skills.
Services in an IFSP may include, but are not limited to:
- Specialized instruction
- Speech therapy
- Occupational therapy
- Physical therapy
If childcare is a part of your child’s regular schedule, services may be able to be provided in the childcare setting, such as a scheduled time for a speech therapist to work with your child during childcare hours, and for childcare staff to include your family’s daily “practice time” to help your child meet their development goals.
If you are just beginning to look for childcare, your FRC may be a good resource to advise you on things to look for and questions to ask to find a childcare setting that can support your family’s IFSP.
You can check out these resources for much more information on Birth-to-3 programs:
Disability Rights for Littles: Key Information for Families of Babies, Preschoolers, and Primary-School Children (videos) -all the basics you need to know
PAVE: From Birth to Three Toolkit Basics and beyond! Read online or download, includes FAQ sheet and “cheat sheets”, summaries of important information at-a-glance.
WA State Department of Children, Youth and Families (DCYF) Early Intervention Services page: Includes contact information and links to apply for an evaluation for ESIT services to find out if your child qualifies.
Individuals with Disabilities Education Act (IDEA), Part B (Age 3 through high school graduation):
IDEA Part B applies to preschool and school-age children, and exists to ensure schools, preschools, and kindergartens provide eligible children with disabilities a Free, Appropriate Public Education (FAPE). When disabilities affect how a child is doing in preschool or school, IDEA Part B states that schools and preschools are required to evaluate the child to see if they qualify for special education and related services and supports. This article from PAVE has important background on this law: IDEA: The Foundation of Special Education.
If a child is eligible for special education, a team is brought together that includes parents, and an Individualized Education Program (IEP) is created for the child, listing the goals, education, and other supports the school or preschool will provide to meet the child’s learning needs.
For childcare settings, IDEA Part B will apply for these types of childcare settings:
- Head Start programs
- Early Childhood Education and Assistance Program
(ECEAP) - Transitional Kindergarten
This PAVE resource explains the differences in services between Part B and Part C of IDEA.
Section 504 of the Rehabilitation Act of 1973
Often called “Section 504” for short, this federal law administered by the Office of Civil Rights prohibits discrimination based on disability. To be protected under Section 504, a child must have a physical or mental impairment that substantially limits one or more major life activities, have a record of such an impairment, or be regarded as having such an impairment.
Section 504 applies to individuals 3-22 years of age. The law requires childcare centers, camps, and any other recreational programs that receive federal funding to provide preschool children with disabilities equal access to the program, with reasonable accommodations and modifications.
It also includes programs like Head Start, summer programs, and extended school day programs.
Requirements for childcare centers:
- Non-discrimination: Childcare centers cannot refuse to admit a child with a disability.
- Reasonable Accommodations: They must provide reasonable accommodations to enable children with disabilities to participate in the program.
- Individualized Assessments: Childcare providers must make an individualized assessment of a child’s needs.
- Modifications to Policies and Practices: They must make reasonable modifications to their policies and practices.
- Accessible Facilities: Childcare centers must ensure that physical spaces are accessible.
Help paying for childcare:
Federal Tax Credit: The child and dependent care credit is a tax credit that may help you pay for the care of eligible children or dependents. This credit is based on your income and the cost of caring for your children or eligible dependents to work, look for work, or attend school.
Seattle has a Child Care Assistance Program.
Washington State offers a program through the Department of Children, Youth, and Families (DCYF):
Working Connections Child Care (WWCC) helps working families pay for childcare. If a family qualifies and chooses an eligible provider, Washington State will pay part of childcare costs. Parents are responsible for any copayment of childcare fees not covered by the state, and those are payable to the provider every month.
- The child or children must live in Washington State
- The family with whom the child lives must live in Washington State
- The family’s income must be at or below 60% of the State Median Income
- The family must have less than $1 million in resources
- Parent or parents must be participating in an approved activity, such as self-employment, employment, or being in high school or post-secondary education or taking part in the WorkFirst or BFET program.
- Families experiencing homelessness are eligible.
- If a parent or parents are seasonal agricultural (farm) workers, and live in certain counties, they may be eligible for the Working Connections program.
An additional up-to-date online resource is MomsRising.org. This site has brief, helpful information about the Working Families Child Care Program, especially when your child or children have a disability. It goes over issues such as:
- How families and family size are defined for this program
- Children with physical, intellectual and/or developmental disabilities
- Children and families experiencing homelessness
- Families where the parent or parents are high school or college students
- What types of childcare are available
- Getting financial assistance when a family member, friend, or neighbor can take care of your child or children
- You can check details of your eligibility, including income requirements, on DCYF’s Working Connections Child Care website page.
- Apply by calling the Child Care Subsidy Contact Center 1-844-26-8687 or online at Washington Connection.
- Get help applying for this program and help finding childcare that meets your family’s needs through ChildCare Aware of WA.
Free state-licensed early learning childcare or preschool:
Head Start programs are federally funded and Early Childhood Education and Assistance Program (ECEAP) is a Washington State-funded program for children aged three and four, and in some locations, infants and toddlers younger than age three. Head Start offers services to pregnant women in some locations.
Your local school district will have an ECEAP program available.
Children are eligible for these programs based on their age and family incomes, with some children able to attend these free programs if they have multiple support needs. Visit the ECEAP & Head Start programs page on the DCYF website for more detail and contact information in English and Spanish.
Financial help for childcare by family, friends, or neighbors:
In Washington, this category is called Family, Friend and Neighbor Care. These settings are not required to have a license and are very common arrangements.
Informal care for children in your home or the family’s home may involve some expenses, and Washington State recognizes this with financial assistance (subsidies). Visit the Family, Friend and Neighbor Care page on DCYF’s website for contact information to apply for subsidies.
Online – Special Education Workshops
May 21 @ 6:00 pm – 7:00 pm PDT
Present Levels & SMART Goals: Connecting the Dots in the IEP
Discover how to align present levels with meaningful, measurable SMART IEP goals that drive progress.
Presenter: Sherry Mashburn
November 20 @ 6-7 PM
Special Education Eligibility: How Schools Decide / Elegibilidad para Educación Especial: Cómo Deciden las Escuelas
Get a clear look at how school districts determine eligibility, the evaluation process, and what it means for your child’s access to special education services. / Obtenga una visión clara de cómo los distritos escolares determinan la elegibilidad, el proceso de evaluación y lo que esto significa para el acceso de tu hijo(a) a los servicios de educación especial.
January 15 @ 6-7 PM
Accommodations, Modifications, and SDI: What’s the Difference?
Discover how to align present levels with meaningful, measurable SMART IEP goals that drive progress.
Presenter: Marie Kerr
February 19 @ 6-7 PM
Discipline in Schools: What Parents Need to Know
Explore how discipline works for students with IEPs, including suspension rules, manifestation determinations, and how schools must balance safety with your child’s rights.
Presenter: Sherry Mashburn
April 23 @ 6-7 PM
High School Transition Planning: Preparing for What’s Next / Planificación de la Transición en la Escuela Secundaria: Preparándose para lo que Sigue
Learn how transition plans prepare your child for life after high school, college, work, and independent living, and how to make sure the plan reflects your child’s voice. / Aprende cómo los planes de transición preparan a tu hijo(a) para la vida después de la escuela secundaria, la universidad, el trabajo y la vida independiente, y cómo segurarte de que el plan refleje la voz de tu hijo(a).
May 21 @ 6-7 PM
Inclusion & Belonging: What Parents Should Know
Learn how inclusionary practices help students with disabilities access the general education classroom, build friendships, and thrive, while benefiting all students.
Presenter: Marie Kerr
No registration is required!
Click to join via zoom! – Meeting ID: 737 702 3071
Free
bfcsepta@yahoo.com
Related Events

Get Ready for School with IEP Essentials
Every student deserves a strong start to the school year. For families of children with disabilities, preparing for school includes reviewing the Individualized Education Program (IEP). The IEP is a legal document and a living plan that outlines the supports and services a student needs to access their education. Families play a key role in shaping the IEP and making sure it works for their child.
A Brief Overview
- The start of a new school year is a great time for families to revisit or begin the IEP process to support their student’s learning.
- If a student doesn’t yet have an IEP, requesting an evaluation is the first step to determine eligibility for special education services.
- Review the IEP before school starts to prepare questions and suggestions for the team.
- Talk with your student about what to expect to reduce anxiety and build confidence.
- Learn about the Individuals with Disabilities Education Act (IDEA) to understand your rights and responsibilities in the IEP process.
- Communicate regularly with the IEP team to monitor progress and adjust plans as needed.
- Gather documents, write questions, and invite support to prepare for IEP meetings.
- Follow up after meetings to confirm next steps and maintain communication.
- Take small, manageable steps to stay involved and support your student’s success.
Introduction
The beginning of a new school year is the perfect time to revisit your student’s Individualized Education Program (IEP). Whether your child already has an IEP or you’re just starting to explore the special education process, this season offers a fresh opportunity to reflect, plan, and engage.
As you and your student get ready for school, the most important thing is the “I” in IEP. The “I” is for “Individualized”. A thoughtful IEP highlights abilities and helps your student access the supports needed to learn. It helps ensure they receive the support necessary to learn, grow, and make meaningful progress—not just in school, but in life beyond graduation.
IEPs are built by teams, and families are essential members. When parents and students understand the process and actively participate, they help shape a plan that truly works.
What to do before the first day
If your student doesn’t have an IEP and you wonder whether a disability might be affecting their learning, now is a great time to explore the special education process. Understanding how evaluations work is the first step. If you’re unsure whether your child needs one, check out our article on How to Request an Evaluation, which explains how to get started.
Before the school year begins, review the IEP to prepare questions and suggestions for the team. PAVE recommends using their Steps to Read, Understand, and Develop an Initial IEP worksheet to guide this process.
After reviewing your student’s IEP or beginning the process to request one, the next step is ensuring your child is properly enrolled in school. Enrollment procedures vary by district, but they typically include submitting documentation, verifying residency, and understanding school assignment policies. For a clear overview of how and when to enroll your student, read this PAVE article: Starting School: When and How to Enroll a Student in School.
To help ease anxiety and build excitement, talk with your child about what to expect. Discuss new activities, classmates, and what will feel familiar. If your school offers an open house, plan to attend together. During your visit, take pictures and ask your child what they notice or wonder about. You can review the photos later to help them feel more prepared. PAVE’s article, Tips to Help Parents Plan for the Upcoming School Year, provides actionable strategies for easing anxiety, fostering independence, and creating a positive school experience.
What parents need to know about FAPE
At the heart of special education is the right to a Free Appropriate Public Education (FAPE), guaranteed by the Individuals with Disabilities Education Act (IDEA). FAPE means that students with disabilities are entitled to an education tailored to their individual needs—not a one-size-fits-all program. This is what makes IDEA unique: it ensures that every eligible student receives services designed specifically for them through an Individualized Education Program (IEP).
To qualify for an IEP, a student must go through an evaluation process to determine if a disability is impacting their education. If the student meets criteria under IDEA, they become eligible for special education services. These services are not about placing a student in a specific classroom—they’re about providing the right support, wherever the student learns. As you review your child’s IEP or prepare for meetings, ask: Is this plan appropriate and suitable for my child’s unique abilities and needs?
IDEA includes six important principles
The IDEA, updated several times since 1990, outlines legal rights for students with disabilities and their families. This PAVE article, Special Education Blueprint: The Six Principles of IDEA, explores the core principles, including: Free Appropriate Public Education (FAPE), Appropriate Evaluation, Individualized Education Program (IEP), Least Restrictive Environment (LRE), Parent and Student Participation, and Procedural Safeguards.
Effective communication is key to student success
Understanding legal rights is just the beginning—clear, consistent communication with the IEP team is one of the most effective ways to ensure your student’s plan leads to meaningful progress. Consider creating a communication plan with your child’s teachers or case manager. This might include weekly emails, a journal sent home in the backpack, scheduled phone calls, or progress reports. Be sure to have this plan written into the IEP or included in the Prior Written Notice (PWN) so everyone stays on the same page.
Writing down how you’d like to stay in touch helps the team understand what works best for your family. Get creative—what matters most is that the plan supports clear, consistent communication for the whole team. Here are a few ideas for ongoing communication with the school:
- A journal that your student carries home in a backpack
- A regular email report from the Special Education teacher
- A scheduled phone call with the school
- A progress report with a specific sharing plan decided by the team
- Get creative to make a plan that works for the whole team!
Keep a log of communication with the school district and educational service providers. PAVE provides a downloadable Communication Log to help you track emails, phone calls, and texts.
Ready, set, go! 5 steps for parents to participate in the IEP process
Understanding the laws and principles of special education can help parents get ready to dive into the details of how to participate on IEP teams. Getting organized with schoolwork, contacts, calendar details, and concerns and questions will help.
This 5-step process is downloadable as an infographic.

Download the IEP Essentials in 5 Steps in:
English | Chinese (Simplified) 中文 (Zhōngwén) | Korean 한국어 (Hangugeo) | Russian Русский (Russkiy) | Somali Soomaali | Spanish Español | Tagalog | Ukrainian українська | Vietnamese Tiếng Việt
1. Schedule
Parents or guardians should receive a written invitation to the meeting. The school and family agree on a date and time, and the school documents efforts to include families at all IEP team meetings. If the proposed time doesn’t work, remember that parents are required members of the team—you can request a different time that works better for you.
Ask beforehand for the agenda and a list of who will attend. This helps ensure there’s enough time to fully address the topics being discussed. If a key team member can’t attend the meeting, you have the option to either provide written consent to excuse their absence or request to reschedule if their participation is important to you. For a list of suggested attendees and a downloadable form to save contact information, PAVE provides a Who’s Who on the IEP Team.
If your student already has an IEP, a re-evaluation occurs at least once every three years unless the team decides differently. A parent can ask for a re-evaluation for sooner if needed, though typically a re-evaluation will not occur more than once a year.
2. Prepare
You can ask for a copy of the evaluation results or a draft IEP before the meeting to help you prepare. It’s a good idea to gather letters or documents from medical providers or specialists that support your concerns. Writing down a few questions ahead of time can help you remember what you want to ask. You might also make a list of your student’s strengths and talents—this helps the team build on what’s already working. If you have specific concerns, you can write a letter and ask for it to be included in the IEP. Some families invite a support person to attend the meeting, someone who can take notes, help you stay focused, and offer encouragement.
3. Learn
Knowing the technical parts of an IEP will help you understand what’s happening at the meeting. The IEP is a living program—not just a document—and it can be updated anytime to better meet your child’s needs. The IEP is a work-in-progress, and the document can be changed as many times as needed to get it right and help everyone stay on track.
Familiarize yourself with the components of an IEP:
- Present levels of performance
- Educational impact statement
- SMART goals (Specific, Measurable, Achievable, Relevant, Timely)
- Services, supports, and placement
- LRE details
- Transition planning (starting by age 16)
- Behavior supports, if needed
- Specially designed Instruction
4. Attend
At the meeting, each person should be introduced and listed on the sign-in sheet. Schools generally assign a staff member as the IEP case manager, and that person usually organizes the team meeting. Any documents that you see for the first time are draft documents for everyone to work on.
Be present and free of distractions so you can fully participate. Ask questions, share your perspective, and help keep the focus on your child’s needs and goals. If your child isn’t attending, placing a photo of them on the table may remind the team to keep conversations student-centered.
Everyone at the table has an equal voice, including you!
5. Follow up
After the meeting, follow through with the agreed communication plan. Make sure that everyone’s contact information is current and that you know how and when updates will be shared. If you still have concerns after the meeting, request a follow-up meeting or submit additional notes.
Stay organized with calendars, contact lists, and copies of important documents. Talk with your child about the upcoming year to ease anxiety and build excitement!
Tips for a smooth school year
As the school year begins, it’s important to think proactively about how to support your child’s learning and development. Establishing routines, setting goals, and building relationships with school staff can make a big difference.
If all of this sounds a little overwhelming, break the work into steps. Determine the best way to help your family stay organized with paperwork and information. Choose a calendar system that helps you track appointments and school events, such as back-to-school night or parent-teacher conferences.
Help your child’s team understand what works best for your student and share their strengths with a one-pager or a letter of introduction. PAVE provides a one-pager template, What You Need To Know About My Child, and a sample letter of introduction, Sample Letter to the IEP Team – Today Our Partnership Begins.
Let’s wrap things up!
Getting ready for school can feel like a lot, especially when your child has an IEP. But you don’t have to do everything at once. Take it one step at a time, and remember: you are not alone. This journey includes your child, and you’re walking it together. You are a vital part of your child’s team, and your voice truly matters. When families and schools work as partners, amazing things can happen. So trust yourself, speak up, and share what you know—because no one knows your child better than you. You bring love, insight, and hope to the table.
From all of us at PAVE, we wish you a happy and successful school year!
Learn More
- PAVE – Placement: Deciding Where a Student Spends the School Day: Understand how placement decisions are made and what options may be available for students.
- PAVE – What Parents Need to Know when Disability Impacts Behavior and Discipline at School: Explains how behavior and discipline are handled within special education and what rights families have.
- PAVE – Toolkits Ready for You!: Offers downloadable guides and checklists to help families stay organized and informed throughout the IEP process.
- Office of the Superintendent for Public Instruction (OSPI) Special Education Resource Library: Provides access to Washington State’s official guidance, forms, and tools for navigating special education.
Developmental Screening (Birth to Three and Medically needed developmental screening)
What is Developmental Screening?
Developmental screening is the practice of systematically looking for and monitoring signs that a young child may be delayed in one or more areas of development. Screening is not meant to establish a diagnosis for the child, but rather to help professionals and families determine whether more in-depth assessment is the next step. By using a high-quality screening tool, professionals can screen children for delays accurately and cost-effectively.
Think about your child’s first months. The medical professionals set up regular “Well-child” appointments just to monitor how your child is doing. These “Well-child” visits allow doctors and nurses to have regular contact with children to keep track of the child’s health and development through periodic developmental screening. Developmental screening is a simple process that can have both informal and formal assessments. When using a tool that is more formal in nature, the short test can tell if a child is learning basic skills when he or she should, or if there are delays. Developmental screening can be done by other professionals in health care, community, or school settings.
We have heard many times over the years that a child’s greatest window for development is in the first five years of life. Eighty-five percent of the brain’s development occurs before age three, making the first years of life critical to a child’s future success. The research shows that early intervention greatly improves a child’s developmental and social skills. Early intervention services help children from birth through 3 years of ages. Services usually include the support of an early educator who works with the family, as well as therapy (if identified as a need) to help the child talk, walk, and interact with others.
It’s not uncommon for parents to become concerned when their little one doesn’t seem to be developing within the normal schedule of “baby” milestones. You may worry that he hasn’t rolled over yet, or that he isn’t doing what the neighbor’s child, who is about the same age is doing. There may be concerns about your baby sitting up or beginning to verbalize words and sounds.
While it’s true that children develop differently, at their own pace, and that the range of what’s “normal” development is quite broad, it’s hard not to worry and wonder. If you think that your child is not developing at the same pace or in the same way as most children his or her age, it is often a good idea to talk to your child’s pediatrician. Explain your concerns. Tell the doctor what you have observed with your child. The doctor or other professionals might ask you some questions they may also talk and play with your child to see how he or she plays, learns, speaks, behaves, and moves. A delay in any of these areas could be a sign of a problem.
You can also get in touch with your community’s lead agency for birth-to-three services, and ask for an evaluation to see if there are possible delays. Based on referrals from the Doctor and the evaluation provided by the early intervention team, your child may be eligible for early intervention services, which will be developed with you and will address your child’s special needs.
Screening is a simple process that can identify infants and young children who may be at risk for health, developmental, or social/emotional problems. It identifies children who may need a health assessment, diagnostic assessment, or educational evaluation. “Screening” means using a standardized instrument. This could include a parent questionnaire, observational process, or other form of measurement that has been validated by research to learn more about the child’s development. Using a standardized instrument is much more effective for identifying real concerns or delays than just using professional judgment or informal questions about the child’s development.
The screening process provides an opportunity for young children and their families to access a wide variety of services and early childhood programs. It also supports the parents’ understanding of their child’s health, development, and learning.
The developmental screening and evaluations can lead to the involvement of a Family Resource Coordinator who will walk with the family through those first three years. They do a family needs assessment, if the family wishes to have one done. This helps identify areas the needs and priorities of the child’s family. Family-directed services are meant to help family members understand the special needs of their child and how to enhance the child’s development.
The need to provide early intervention is significant. Many children with developmental delays are not being identified as early as possible. This can result in these children waiting to get the help they need to do well in social and educational settings until they are in a school or pre-school setting. Research has shown that in nearly one in six Washington kids has a developmental delay, but only 30% of these children are identified before starting kindergarten, when early support services are most effective. Additionally, research has also identified that in the United States, about 13% of children 3 to 17 years of age have developmental or behavioral disabilities. These can include autism, intellectual disabilities, and attention-deficit/hyperactivity disorder. Additionally, there are children who have delays in language, social skills, or other areas that affect school readiness. This same research found that many children with developmental disabilities weren’t identified before age 10. These types of delays have significant implications since by that age there are significant delays that might have been addressed earlier and provided opportunities for services and support that was missed.
Because of the rapid growth in a child’s first three years of life, early support and monitoring of child development is essential for these children to reach their full academic potential as well as social and personal success. In all cases, kids will experience greater success academically, socially, and personally if delays are caught early and kids and families get the support they need. Free developmental screening using the Ages and Stages Questionnaire-3 screening tool is one of the best ways to get more awareness of what can help your child. In addition to the Ages and Stages survey a terrific tool and support network has been established called “Within Reach”. The “WithinReach” website is committed to supporting optimal child development of all Washington families. Through the “WithinReach” Family Health Hotline and Plan a Save Care (POSC), families can access free developmental screening, connections to early learning and family support and referrals to early intervention for developmental delays.
If you would like a free developmental screening for your child or have concerns about your child’s development, it is as easy as calling their Family Health Hotline (800) 322-2588 or visiting their website at www.ParentHelp123.org.
Remember that as important as Developmental screening is as a part of early intervention, can go also be important in assuring that the needs of children of older ages also find success and resources. Developmental screening for older youth can include areas of the individual’s development in mental health, social and emotional needs, and communication needs, just to name a few. Developmental screening will help assure that the needs of the individual whether an infant or an older child, can be met, and how those needs can be met. As parents and family members we have a responsibility to help our children thrive and developmental screening can help us know which path to follow to make that happen.
Resources for this article:
Overview of Early Education from Center for Parent Information & Resources
Within Reach – Want to learn more about your child’s development?
Ages and Stages Questionnaires – Helping parents understand the Benefits for Developmental Screening
CDC- Developmental Monitoring and Screening
CDC – Autism Spectrum Disorder (ASD)
CDC – Facts about intellectual Disability
Getting to Know the Individualized Family Service Plan (IFSP)
The Individualized Family Service Plan (IFSP) is an essential tool designed to support infants and toddlers with developmental delays or disabilities. This guide provides a structured overview of each step in the companion worksheet, breaking down the IFSP process and essential actions family caregivers should take.
Brief Overview
- Part C of the Individuals with Disabilities Education Act (IDEA) ensures the right to early intervention services for infants and toddlers (birth to age three) with developmental delays or disabilities.
- Washington’s Department of Children, Youth, and Families (DCYF) administers early intervention services to eligible children in the state through Early Support for Infants and Toddlers (ESIT).
- The Individualized Family Service Plan (IFSP) is a comprehensive, whole family plan to provide tailored services and supports.
- Parents and family caregivers play a crucial role in the IFSP process and have the right to be fully involved.
- PAVE provides a fillable Getting to Know the Individualized Family Service Plan (IFSP) Checklist for download in multiple languages.
Download the: Getting to Know the Individual Family Service Plan (IFSP) Checklist
English | Spanish Español |
Introduction
Part C of the Individuals with Disabilities Education Act (IDEA) protects the rights of infants and toddlers with disabilities, from birth to age three, who qualify for early intervention services. In Washington, the Department of Children, Youth and Families (DCYF) administers services for eligible children through Early Support for Infants and Toddlers (ESIT). Children who qualify receive services through an Individualized Family Service Plan (IFSP).
An IFSP is a comprehensive plan designed to support infants and toddlers with developmental delays or disabilities. It outlines the child’s current levels of development, sets specific goals, and details the services and supports needed to achieve these goals. The IFSP also includes information about the child’s family and their resources, priorities, and concerns, ensuring that the plan is tailored to the family’s unique situation. Additionally, it specifies the frequency, intensity, and method of the services to be provided, along with the professionals responsible for delivering them. The plan is reviewed every six months and is updated at least once a year but can be reviewed at any time by request of parents or other team members. The review process involves discussing:
- Progress toward existing goals
- Whether services should continue, increase, or decrease
- Any new concerns that need to be addressed
Step 1: Read the IFSP draft before the IFSP meeting.
Ask for a copy of the IFSP draft in advance of the meeting. Getting the draft before the meeting gives you time to read through it and understand what is being proposed. If you prepare and know what will be discussed, you will feel more confident and involved in the planning process. This will also help you give better feedback during the meeting.
Review the document carefully to ensure all necessary information is included. Take your time to go through each section of the IFSP draft. Make sure that the details about your child and their needs are correct and clearly stated. Look for any missing information or areas that need more explanation.
Understanding the IFSP is crucial for making informed decisions about your child’s care. Under state and federal law, parents have the right to information about their child’s education in a language they can understand. If English is not your first language, ask for a translation so you can fully understand the document. This ensures that you can participate effectively in the meeting and advocate for your child’s needs.
Step 2: Review your child’s present levels and needs.
After a child is evaluated, data are compared against typically developing children of the same age. If scores show a 25 percent delay overall or if the score in one developmental area is statistically 1.5 standard deviations below typical peers, then the child is eligible for an IFSP. Your child’s present level of development will include a developmental level, including the percentage of delay, for each of the developmental areas evaluated.
ESIT uses standardized tools and observations to evaluate a child’s development in five areas: physical, cognitive, social-emotional, communication, and adaptive. Physical skills include fine motor and gross motor development, including movement and coordination. Cognitive skills involve thinking and learning. Social-emotional skills are about interacting with others and managing emotions. Communication skills cover understanding language (receptive) and using language (expressive). Adaptive skills are daily living activities like dressing and eating. Your child may also be evaluated for vision and hearing development. Assessing these areas gives a complete picture of your child’s development and helps guide the support they need.
Carefully read the summary of your child’s functional performance to identify their social-emotional, communication, and behavioral strengths. By knowing their strengths, you can build on them to help your child grow. This means identifying areas where your child excels and using these strengths as a foundation for further development. For example, if your child has strong fine motor skills, you can incorporate activities that involve drawing, building with blocks, or holding eating utensils. Recognizing and leveraging strengths can boost your child’s confidence and motivation, making learning more enjoyable. It also helps create a more balanced and positive approach to their development, focusing not only on areas of need but also on celebrating and expanding their abilities.
Understanding your child’s weaknesses will allow you to focus on areas that need improvement. Based on the evaluation data, the IFSP will identify what specific supports and services your child requires. These needs might include therapies, special education, or other interventions. For example, if your child has cognitive delays, the plan might include early intervention services that focus on developing problem-solving and learning skills. This could involve activities like puzzles, matching games, or simple counting exercises that help your child improve their cognitive abilities.
Step 3: Read the family priorities and concerns for accuracy.
The IFSP is a whole family plan, with the child’s primary caregivers as major contributors to its development and implementation. Carefully read the sections that refer to family priorities and concerns. Write down anything you would like to add or change.
The IFSP includes goals, and progress is monitored to determine whether the plan is supporting appropriate outcomes. The plan is reviewed every six months and is updated at least once a year but can be reviewed at any time by the request of parents or other team members.
As you think of additional concerns and priorities, make note of them to discuss at the IFSP meeting. Every six months, or whenever necessary, the IFSP can be adjusted to reflect new developments, emerging needs, or changes in family priorities. Urgent or time-sensitive issues do not have to wait until the six-month review. Family caregivers can request a meeting to discuss their concerns or update the IFSP at any time.
Step 4: Review any recommended resources.
Explore the community resources and supports listed by the Family Resource Coordinator (FRC). Some may require additional application processes and paperwork. Begin by identifying which resources are most important and the starting point to connect with their services or information. Plan to work through each step and make note of those resources that you want to explore further.
Step 5: Consider the major results/outcomes expected of your child.
The IFSP outlines specific outcomes, or goals, based on the child’s present levels of development. Review the outcomes outlined for your child’s development. The outcomes should be practical and fit into daily routines, and they should be written so the IFSP team can measure progress.
Some skills require gradual learning. If a goal seems too broad or complex, breaking it into smaller, manageable steps (or “chunking”) can make it easier for the child to achieve success. For example, if the goal is for a child to use a spoon independently, the steps might include:
- Holding the spoon correctly
- Scooping food with assistance
- Practicing controlled movements to the mouth
- Eating independently with minimal spills
Write down your concerns and observations about specific outcomes to discuss with the IFSP team. If a goal is too ambitious or not challenging enough, adjustments can be made to better fit your child’s pace of development.
Step 6: Identify the services, including frequency and duration.
Early intervention services are designed to meet the child’s individual needs. Locate your child’s services, the frequency and duration, and the outcomes related to each service. Review the types of services your child will receive, such as speech therapy or occupational therapy, and whether they will be provided individually or as part of a group.
Step 7: Review the location(s) of service delivery.
Services are typically provided in the child’s home or other natural environment, where everyday learning opportunities occur, such as their home or daycare. They also can be offered in a medical hospital, a clinic, a school, or another community space. Any services provided outside the child’s natural environment require a statement explaining the rationale for the placement, including why an outcome cannot be achieved in a natural environment and a plan to move the service or support into the natural environment.
Review the location(s) where your child will receive their services and note any concerns you have, including issues with accessibility, transportation, and distance from their natural environment.
Step 8: Identify the source of funding or payment for services.
Washington State provides most early intervention services at no cost to families of eligible children. Some services covered by insurance are billed to a child’s health insurance provider, with the signed consent of a family caregiver. The early intervention system may not use health care insurance (private or public) without express, written consent. The IFSP will include any payment arrangements for services that are not covered by Part C.
Part C of the IDEA requires states to provide the following services at no cost to families: Child Find (outreach and evaluation), assessments, IFSP development and review, and service coordination.
Step 9: Save your FRC’s information.
The FRC is your main contact for your child’s early intervention services. The IFSP lists the FRC’s name and contact information. If you have any concerns or disagree with any part of the process, you can reach out to your FRC at any time for help and guidance with accessing services. While your child is receiving early intervention services, communicate any updates or additional support needs to your FRC.
Final Thoughts
As a parent or caregiver, you have the right to be fully involved in your child’s early intervention journey. Following these steps ensures that families are well-prepared to navigate the IFSP process. Understanding the IFSP process gives you the knowledge and confidence to make informed decisions, ensuring your child receives the best possible support for their development. By staying informed, actively engaging with the IFSP team, and advocating for their child’s needs, families can help create an effective and supportive early intervention plan for their child’s development.
Learn More
Beyond School Walls: A Guide to Homeschooling in Washington State
Homeschooling is a popular and flexible educational option for many families. “Home-based instruction” (HBI), as it’s referred to in Washington State law, must meet specific required subjects and instructional hours (or school days) annually. If you’re considering homeschooling, it’s important to understand the legal requirements and steps involved, including the qualifications that make a parent or guardian eligible to provide home-based instruction. Homeschooled students can access public school resources like extracurricular activities, part-time classes, and even special education services. By understanding and adhering to these guidelines, you can ensure a successful and enriching homeschooling experience for your child.
A Brief Overview
- Homeschooling or home education programs are called “home-based instruction (HBI)” in Washington state.
- A parent or guardian must meet one of four qualifying criteria to homeschool, or register through an approved private school extension program.
- Homeschooling must cover 11 required subjects and at least 1,000 instructional hours annually (or 180 school days), but Washington law (RCW 28A.200.020) allows for flexibility in teaching methods and curriculum selection, emphasizing a personalized approach.
- Beginning on their eighth birthday, your child must be enrolled in a school or home-based instruction, in accordance with Washington’s compulsory attendance law (RCW 28A.225.010).
- If your student was enrolled in school prior to homeschooling and they are 8 years of age or older, they must be withdrawn by written and signed statement, and you must file a Declaration of Intent with your local public school district. The Declaration of Intent must be filed by September 15th annually, or within two weeks of the beginning of the public school year.
- Homeschooled children must complete yearly assessments, either through standardized testing or an evaluation by a certificated educator. Parents and guardians must keep the results in their homeschooling files as a permanent record.
- Families can request a special education evaluation from the public school district regardless of whether their child is enrolled in public school. If the child is eligible, the district must provide ancillary services unless the family declines them (RCW 28A.150.350).
- Homeschooled students can participate in public school resources, including part-time enrollment in virtual or in-person classes, extracurricular activities, and sports.
- PAVE provides a downloadable Annual Checklist for Home-Based Instruction to help families maintain compliance with Washington’s homeschool statutes.
Introduction
Whether you are looking for an alternative to public school or continuing a home education program you began before moving from out of state, there are some things you need to know before homeschooling your student in Washington State. Homeschooling, referred to as “home-based instruction (HBI)” in the state statutes, comes with specific guidelines and requirements.
To homeschool, a parent or guardian must:
- Meet the qualifications for homeschooling under state law (RCW 28A.225.010(4))
- Provide 180 school days or 1,000 instructional hours annually in the 11 required subjects
- Formally withdraw the student from public school
- Notify the school district of annually with a Declaration of Intent
- Have the student complete an annual test or assessment
- Maintain homeschool records
What qualifications must a parent or guardian meet to homeschool?
A parent or guardian has to meet one of the following qualifications to homeschool their child:
- Hire a certified teacher to supervise the instruction.
- Complete 45 college quarter credits or the equivalent in semester credits.
- Complete a course in home-based education, sometimes referred to as a parent qualifying course, at a postsecondary or vocational-technical institute.
- Gain approval from the superintendent as “sufficiently qualified to provide home-based instruction.” Those who have homeschooled in another state and move into Washington may be more successful with this by demonstrating a documented history of homeschooling.
If you do not meet these qualifications, you may homeschool through a private school extension program. Locate an approved private school that allows the homeschooling option and contact the school directly.
What do homeschool students learn?
Washington law mandates that homeschooled children receive at least 1,000 instructional hours annually (or 180 school days), similar to the public school system. There are 11 required subjects, although parents do not have to teach every subject daily, weekly, or even yearly. Some subjects, like social studies, are for younger grades, while others, like history, are for older grades. The homeschool curriculum must include the following subjects:
- Occupational education
- Science
- Math
- Language
- Social studies
- History
- Health
- Reading
- Writing
- Spelling
- Art and music appreciation
You have full control over your homeschooling curriculum, allowing you to tailor the education to your child’s needs and interests. You are responsible for decisions related to educational philosophy, selection of books, teaching materials, curriculum, and methods of instruction (RCW 28A.200.020).
Washington law acknowledges that “home-based instruction is less structured and more experiential than the instruction normally provided in a classroom setting.” As a result, the nature and quantity of instructional and educational activities are “construed liberally”. This flexibility gives you the freedom to create a personalized educational experience. (RCW 28A.225.010(5))
When and how can I withdraw my student from public school?
Children living in Washington must be enrolled in a school or home-based instruction starting on their eighth birthday. The law requires compulsory attendance from age eight until eighteen (RCW 28A.225.010). Any educational programs your child participates in before age eight are not subject to state requirements for home-based instruction.
If your child is enrolled in a public or private school and you decide to homeschool, you must first formally withdraw your student. This process involves submitting a withdrawal form provided by the school or a written statement including the student’s name, school name, date of withdrawal, your signature, and the date of signing.
If your child is 8 years of age or older, notify the school district of your intent to homeschool on the same day that you withdraw them from public school, even if they have not yet begun classes or an educational program at the school.
How do I notify the school district that I am homeschooling my child?
For every school year that your child is homeschooled, you must file a written statement, called a Declaration of Intent, with the district superintendent. The address of the superintendent is usually the district office, which you can find on the school’s website or by calling your local school. You may retain a district-stamped copy of the Declaration of Intent by including a second copy and a self-addressed envelope with prepaid postage in your mailer. The deadline to file is September 15th or within two weeks of the beginning of the public school year.
A Declaration of Intent is not required for children who begin school before age 8. For example, a 5-year-old who has started kindergarten may be withdrawn for home-based instruction. The child started going to school before compulsory attendance applied. As a result, the parent is not required to file a Declaration of Intent. If you intend to start your student’s educational career in homeschool, submit your first Declaration of Intent when your child turns 8 years old and compulsory education begins.
The Office of Superintendent of Public Instruction (OSPI) has provided a Sample Declaration of Intent that includes all of the required information: the child’s name, age, address, and parent’s name. This documents that the parent is complying with compulsory education requirements, and the student is receiving an education. The Declaration of Intent must also specify whether a certified teacher will supervise the instruction.
What are my options to complete the required annual assessments?
There are two options for the required annual assessments:
- Standardized Test: Administered annually by a qualified individual approved by the test publisher. The test must be a standardized academic achievement test recognized by Washington State Board of Education (SBE). For a list of examples of tests, see the SBE Home Instruction FAQs page.
- Annual Assessment: Conducted by a certificated person currently working in the field of education. The evaluation must be written. Washington law does not provide as much detail about the criteria for evaluations, but it should include “statements and documents that reflect the child’s progress, or lack thereof” (OSPI).
The purpose of the annual test or evaluation is to provide an external metric to measure a student’s progress. The results are for the parent’s use only, unless the child is later enrolled at a public or private school. Parents can choose either option each year based on what works best for their child. Keep the test results in your permanent homeschool record.
Homeschooled students may take part in standardized testing at the public school. The testing dates for the year are usually available at the school office by late September and parents can call the assessment coordinator at the school district to register their student for these tests. Be sure to request a copy of the test scores for your homeschooling file during registration for the standardized test.
If a homeschooled student performs poorly on a test or assessment and the results indicate that they are “not making reasonable progress consistent with his or her age or stage of development,” the parent or guardian is expected to “make a good faith effort to remedy any deficiency”. (RCW28A.200.010(1)(c))
What records do homeschooled students have?
Maintaining good records is an essential part of homeschooling in Washington state, serving as proof of education and compliance with state laws. While the law does not specify the exact form records should take, there are several types of documentation that are meaningful for homeschooled students:
- Attendance records tracking the 180 school days or 1,000 instructional hours required
- Curriculum information documenting the textbooks and workbooks used
- Student work samples and portfolios demonstrating application of what they’ve learned
- Communication with school officials, including the annual Declaration of Intent and proof of mailing, such as the Certified Mail-Return Receipt
- Test results, such as annual standardized tests and assessments
- Immunization records
These records can be requested by school administrators if your child later enrolls in a traditional school setting. You should permanently keep proof of compliance with home education laws, including the Declaration of Intent and results of the annual assessments. Homeschool Legal Defense Association (HSLDA) recommends keeping all records from your student’s high school years because they may be requested as proof of education by a post-secondary education program, upon joining the military, or as part of an employment-related background check.
Does the public school have to provide special education and related services to homeschooled students?
Families have the right to request an evaluation for special education from the public-school district regardless of whether a child attends public school. If the child is found eligible, the local district is responsible for providing services unless the family does not want them. In some cases, families arrange to have a child attend private or home-based school but receive special-education services through the public school. These special education services are known as “ancillary services” and they are defined in Washington Administrative Code (WAC) as “any cocurricular service or activity, any health care service or activity, and any other services or activities, except ‘courses,’ for or in which preschool through twelfth grade students are enrolled by a public school” (WAC 392-134-005).
Ancillary services include but are not limited to:
- Therapies, such as counseling, speech and hearing therapy
- Counseling and health services
- Testing and assessments
- Supplementary or remedial instruction
- Tutorial services, which may include home or hospital instruction
- Sports activities
According to The Pink Book: Washington State Laws Regulating Home-Based Instruction, available on OSPI’s Home-Based Instruction page, the definition of “course” specifies that a service or activity meets all of the requirements of an ancillary service but is instructional in nature.
Can homeschooled students take part in public school classes or activities?
Students homeschooled in Washington have access to public school resources, including standardized testing, extracurricular activities, and specialized programs. Families can enroll their children as part-time students to access specific classes or services that complement their home-based instruction (RCW 28A.150.350(d)). Homeschooled students can attend virtual and online public school programs on a part-time basis without losing their homeschool status.
Access to extracurricular activities includes participation in sports and other interscholastic competitions through the Washington Interscholastic Activities Association (WIAA). Homeschooled students are considered “regular members” as long as they have met the State’s home-based instruction requirements, and –
- Annually file a WIAA Rule 18.6.3 form with the principal’s office where the student is enrolled part-time. This form is available on the WIAA website, on the Student Eligibility Center page in multiple languages.
- Do not receive assistance from the school district, and the school district does not receive funding for the student.
- Meet both WIAA and the local school district eligibility requirements.
- Follow transfer rules if they change schools after registering as a homeschool student.
- Provide acceptable documentation of any interscholastic eligibility standards required of all other student participants.
- Comply with WIAA and local school district regulations during participation.
- Adhere to the same team responsibilities and standards of behavior and performance as other team members.
- Participate as a member of the public school in the service area where they reside.
Final Thoughts
Homeschooling in Washington State provides families with a flexible and personalized approach to education while adhering to the state’s legal requirements. By understanding and meeting the necessary qualifications, maintaining proper records, and fulfilling annual assessment obligations, parents and guardians can ensure their child’s education remains compliant and effective. The wide array of resources, from specialized classes to extracurricular activities, further supports a well-rounded learning experience. Whether you are new to homeschooling or continuing from another state, Washington’s supportive framework allows for a rich and adaptable educational journey tailored to each child’s unique needs.
Simple Instructions on How to Get Help From PAVE!
How to Get Help from PAVE (Simple Instructions)
This page shares a short video that shows how to request help from PAVE. If you prefer not to watch the video, a text version of the instructions is included below.
Text version (step-by-step)
- Go to wapave.org.
- Select Get Help.
- Scroll to Select your role, then choose the option that best fits you.
- Fill out the support request form (fields marked with an asterisk * are required). Be sure to include your name and at least one way to contact you (phone and/or email).
- Complete the “I’m not a robot” check (CAPTCHA), then select Submit.
- After you submit, check your email and voicemail for a response from PAVE.
Accessibility note: Captions are available in the video player. A transcript is not posted on this page, but PAVE can provide one upon request (and can share information in another format if needed).
Need Help Another Way?
- If you can’t use the online form, you can contact PAVE by phone or email.
- Share your name, the best way to reach you, the best time to call, and a short description of what you need help with.
- If your situation is an emergency, call 911.
Early Intervention: How to Access Services for Children Birth to 3 in Washington
New parents often worry about their child’s growth and development, especially when comparing with other children. Early intervention can be crucial for children with developmental delays or disabilities. In Washington, families can connect with a Family Resource Coordinator (FRC) for guidance and access free developmental screenings. The Department of Children, Youth and Families (DCYF) offers services through Early Support for Infants and Toddlers (ESIT), providing evaluations and individualized plans (IFSP) to support eligible children from birth to age three. These services, protected under the Individuals with Disabilities Education Act (IDEA), are typically free and aim to help children thrive in various settings.
A Brief Overview
- PAVE provides downloadable toolkits specifically designed for parents and families of young children, including From Birth to Three Toolkit and Transition Toolkit for Ages 3-5.
- Families concerned about a child’s development can call the Family Health Hotline at 1-800-322-2588, with support in multiple languages. Parents can complete a free developmental screening online at Parent Help 123.
- Washington’s Department of Children, Youth and Families (DCYF) administers family-focused services for eligible children from birth to age 3 through Early Support for Infants and Toddlers (ESIT).
- The Individualized Family Service Plan (IFSP), funded by Part C of the Individuals with Disabilities Education Act, is a whole family plan developed with input from caregivers and professionals. It includes goals, services, and progress monitoring, and is reviewed regularly.
- To qualify, a parent must provide written permission for ESIT to conduct an early intervention evaluation of their child. If the evaluation results indicate that the child has a developmental delay or disability, ESIT will develop an IFSP. PAVE provides a Next Steps Checklist: When Your Child is Found Eligible for Early Intervention Services (EIS).
- Early intervention services (EIS) are designed to meet the child’s individual needs, including various therapies and support services. Services are typically provided in the child’s home or other natural environments.
- Various dispute resolution options are available, including mediation and due process. Parents can contact their ESIT Family Resource Coordinator (FRC) if they have concerns or disagreements.
- Most early intervention services are provided at no cost to families. Some services may be billed to insurance with family consent, but certain services are always free under IDEA.
- Active-duty servicemembers whose dependents receive EIS must enroll in the Exceptional Family Member Program (EFMP) for their branch, or the Coast Guard’s Special Needs Program (SNP).
Introduction
New parents may struggle to know whether their child’s growth and development are on track. They may have a feeling that a milestone is missed, or they may observe siblings or other children learning and developing differently. Sometimes a parent just needs reassurance. Other times, a child has a developmental delay or a disability. In those cases, early interventions can be critical to a child’s lifelong learning.
Seek guidance from a Family Resource Coordinator (FRC)
Washington families concerned about a young child’s development can call the Family Health Hotline at 1-800-322-2588 (TTY 1.800.833.6384) to connect with a Family Resource Coordinator (FRC). Support is provided in English, Spanish and other languages. Families can access developmental screening online for free at HelpMeGrow Washington.
Several state agencies collaborated to publish Early Learning and Development Guidelines. The booklet includes information about what children can do and learn at different stages of development, focused on birth through third grade. Families can purchase a hard copy of the guidelines from the State Department of Enterprise Services. A free downloadable version is available in English, Spanish, and Somali from DCYF’s Publication Library. Search by title: Washington State Early Learning and Development Guidelines, or publication number: EL_0015.
Washington early intervention services are provided by ESIT
In Washington, the Department of Children, Youth and Families (DCYF) administers services for eligible children from birth to age 3 through Early Support for Infants and Toddlers (ESIT). Families can contact ESIT directly, or they can reach out to their local school district to request an evaluation to determine eligibility and consider what support a child might need. The ESIT website includes videos to guide family caregivers and a collection of Parent Rights and Leadership resources, with multiple language options.
Early intervention services (EIS) are provided in the child’s “natural environment,” which includes home and community settings where children would be participating if they did not have a disability. According to ESIT, “Early intervention services are designed to enable children birth to 3 with developmental delays or disabilities to be active and successful during the early childhood years and in the future in a variety of settings—in their homes, in childcare, in preschool or school programs, and in their communities.”
Early services are delivered through an IFSP
Children who qualify receive services through an Individualized Family Service Plan (IFSP). The right to an IFSP is protected by Part C of the Individuals with Disabilities Education Act (IDEA). The IDEA is a federal grant program that provides funding for states to implement early learning and special education programs. Part B of the IDEA protects an eligible school-age student’s right to an Individualized Education Program (IEP). Part A includes general guidance about the educational rights of children 0-22.
Family caregivers, childcare professionals, teachers, or anyone else can refer a child for an early learning evaluation if there is reason to suspect that a disability or developmental delay may be impacting the child’s growth and progress. The school district’s duty to seek out, evaluate and potentially serve infants, toddlers or school-aged students with known or suspected disabilities is guaranteed through the IDEA’s Child Find Mandate.
First Step: Evaluate to determine eligibility
Early intervention is intended for infants and toddlers who have a developmental delay or disability. Eligibility is determined by evaluating the child (with parental consent) to see if the little one does, in fact, have a delay in development or a disability. Eligible children can receive early intervention services from birth to the third birthday. PAVE provides an article that describes What Happens During an Early Intervention Evaluation, and a checklist for When Your Child is Found Eligible for Early Intervention Services (EIS).
Next Step: Develop a service plan
If an infant or toddler is eligible, early intervention services are designed to meet the child’s individual needs. Options might include, but are not limited to:
- Assistive technology (devices a child might need)
- Audiology or hearing services
- Speech and language services
- Counseling and training for a family
- Medical services
- Nursing services
- Nutrition services
- Occupational therapy
- Physical therapy
- Psychological services
Services are typically provided in the child’s home or other natural environment, such as daycare. They also can be offered in a medical hospital, a clinic, a school, or another community space.
Individualized Family Service Plan (IFSP): What is the plan?
The IFSP is a whole family plan, with the child’s primary caregivers as major contributors to its development and implementation. Parents/custodial caregivers must provide written consent for services to begin. In Washington, Family Resource Coordinators (FRCs) help write the IFSP. Team members may include medical professionals, therapists, child development specialists, social workers, and others with knowledge of the child and recommendations to contribute.
The IFSP includes goals, and progress is monitored to determine whether the plan is supporting appropriate outcomes. The plan is reviewed every six months and is updated at least once a year but can be reviewed at any time by request of parents or other team members. The IFSP includes:
- The child’s current developmental levels and needs in physical, cognitive, communication, social/emotional, and adaptive areas
- Family information: resources, priorities, and concerns of parents/caregivers.
- Major results/outcomes expected from the child and family
- Specific services:
- Where services are provided—any services provided outside the child’s “natural environment” of home/daycare/community require a statement explaining the rationale for the placement
- When the child receives services—the number of days or sessions for each service, and how long each session will last
- Who pays for the services
- Name and contact information for the Family Resource coordinator (FRC) responsible for IFSP implementation
- Steps to begin at age 2.5 to support the child’s transition out of early intervention and perhaps into school-based services.
- If relevant, additional services or information for the family—such as financial guidance or parenting support
PAVE provides a downloadable checklist to help parents familiarize themselves with the IFSP.
Dispute resolution options are available
If parents have a concern or disagree with any part of the early intervention process, they can contact their Family Resource Coordinator (FRC). If issues remain unresolved, families may choose from a range of dispute resolution options that include mediation, due process, and more. ESIT provides access to a downloadable parent rights brochure with information about dispute resolution options in multiple languages.
Most services are free to families
Washington State provides most early intervention services at no cost to families of eligible children. Some services covered by insurance are billed to a child’s health insurance provider, with the signed consent of a family caregiver. The early intervention system may not use health care insurance (private or public) without express, written consent.
Part C of the IDEA requires states to provide the following services at no cost to families: Child Find (outreach and evaluation), assessments, IFSP development and review, and service coordination.
Early intervention services for military families
Military-connected infants and toddlers receiving early intervention services must be enrolled in the Exceptional Family Member Program (EFMP) while their servicemember is on active-duty orders. The Exceptional Family Member Program (EFMP) is a mandatory program for all branches of the U.S. Armed Forces that helps military dependents with special medical or educational needs. The Army, Navy, Air Force, Marine Corps, and Space Force each have an EFMP and the Coast Guard, which operates under the authority of the Department of Homeland Security, has a similar program called the Special Needs Program (SNP).
The Early Childhood Technical Assistance Center (ECTA), funded by the U.S. Department of Education’s Office of Special Education (OSEP), builds state and local capacity to improve outcomes for young children with disabilities and their families. Military-connected families and others relocating or living outside of Washington State can contact the early intervention services program in their new state with the help of ECTA’s Early Childhood Contacts by State directory.
Military families moving from or to installations that have Department of Defense Education Activity (DoDEA) schools will receive their early intervention services from Educational and Developmental Intervention Services (EDIS). Referrals may come to EDIS from any military medical provider or the parents. Upon receipt of a referral to EDIS, an initial service coordinator is assigned to contact and assist the Family. The initial service coordinator gathers information to understand the family’s concern, shares information about early intervention, and makes arrangements to proceed with the process. In EDIS, any member of the early intervention team can serve as an initial service coordinator. EDIS is provided in locations where DoDEA is responsible for educational services, including some installations on the eastern side of the United States.
Learn More
PAVE provides downloadable toolkits specifically designed for parents and families of young children:
- From Birth to Three Toolkit: This toolkit provides places to begin if caregivers suspect that a baby or young child may need services due to a developmental delay or disability.
- Transition Toolkit for Ages 3-5: This toolkit encompasses a collection of our informative articles, complemented by sample letters to provide you with a solid foundation as you navigate through this crucial transition period.
For additional information:
- The Learn the Signs. Act Early. website provides tools for tracking milestones and materials for families to learn more and plan home-based activities that promote skill development. “Early intervention services can change a child’s developmental path and improve outcomes for children, families, and communities,” the CDC encourages. “Help your child, help your family! Families benefit from early intervention by being able to better meet their children’s needs from an early age and throughout their lives.”
- Check the PAVE calendar for trainings and events, including the Starting Strong webinar about how IDEA supports the rights of infants and toddlers with developmental delays or disabilities and their families.
- PAVE provides an article for next steps after age 3: What’s Next when Early Childhood Services End at Age 3? Another PAVE article for families new to special education: Steps to Read, Understand, and Develop an Initial IEP.
Procedural Safeguards: Student and Parent Rights in Special Education
A Brief Overview:
- Procedural safeguards are a legal requirement for schools and must be provided to parents once a year and during specific situations (e.g., initial referral, filing a complaint, change in placement due to disciplinary action).
- The Office of Superintendent of Public Instruction (OSPI) issued a statewide procedural safeguards notice, available for download in multiple languages, that outlines parental rights in special education.
- The Individuals with Disabilities Education Act (IDEA) requires that each state education agency provide ways to solve disagreements between parents and schools regarding a student’s special education. Procedural safeguards provide information on the formal and informal dispute resolution options available in Washington state.
- Specific protections are in place when disciplining students with disabilities, including requirements for conducting manifestation determinations and continuing education services during extended removals.
- Section 504 includes its own procedural safeguards to protect the rights of students with disabilities who are not eligible for special education under IDEA. The Section 504 Notice of Parent Rights is available for download in multiple languages from OSPI.
Full Article
The Procedural Safeguards are a written set of legal protections under the Individuals with Disabilities Education Act (IDEA) designed to ensure that students with special needs receive appropriate education. IDEA, implemented under Washington State law, requires schools to provide the parents/guardians of a student who is eligible for or referred for special education with a notice containing a full explanation of the rights available to them (WAC 392-172A-05015). Understanding these safeguards allows for effective advocacy in a child’s education and ensures their rights are protected throughout the special education process. They do not constitute legal representation or legal advice.
A copy of the procedural safeguards notice is downloadable in multiple languages from the Office of Superintendent of Public Instruction (OSPI). School districts must provide this notice once a year and during key times such as:
- At the initial referral for special education evaluation and at least once every year after.
- Upon receipt of the first special education complaint or due process hearing request filed by a parent or guardian in a school year.
- When a school decides to remove a student for more than 10 school days in a year through exclusionary discipline, and that removal constitutes a change in placement.
- Any time a parent, guardian, or student aged 18 or older requests them.
In addition to detailing when the procedural safeguards notice must be provided, the procedural safeguards contain information about several key areas, including:
Prior Written Notice
Schools must give prior written notice (PWN) before making any significant decisions about a student’s education, such as changes in identification, evaluation, or placement. This notice must include a detailed explanation of the decision and the reasons behind it. This document is shared after a decision is made and prior to changes in a student’s educational program.
Parental Consent
Schools must get written parental consent (permission) before conducting an initial evaluation or providing special education services for the first time. Parents can withdraw their consent at any time, but this doesn’t undo actions already taken. Once consent is given, the school has 35 school days to complete the evaluation. This consent is only for the evaluation, not for starting services. If the child is a ward of the state, consent might not be needed under certain conditions. When starting special education services under the initial IEP, the school must get consent again, and if refused, they can’t force it through mediation or legal action. Consent is also needed for reevaluations involving new tests, and schools must document their attempts to get it. However, consent isn’t needed to review existing data or give standard tests that all students take.
Independent Educational Evaluation
If a parent disagrees with the school’s evaluation of their child, they can ask for an independent educational evaluation (IEE) that the school district will pay for. The district must give the parent information on where to get an IEE and the rules it must follow. If the district does not agree to the IEE, they have 15 calendar days to either start a file a due process hearing request or agree to pay for the IEE. PAVE provides a downloadable sample Letter to Request an Independent Educational Evaluation.
Confidentiality of Information
Student educational records are confidential. IDEA provides parents and guardians the right to inspect and review their student’s educational records and request amendments if they believe they are inaccurate or misleading. When the child turns 18 years of age, these rights pass from the parent or guardian to the student. The Department of Education provides a website page called Protecting Student Privacy to share resources and technical assistance on topics related to the Family Educational Rights and Privacy Act (FERPA). The procedural safeguards explain terms about educational records from IDEA and FERPA to help parents understand their rights and protections.
Dispute Resolution
IDEA requires that each state education agency provide ways to solve disagreements between parents and schools regarding a student’s Individualized Education Program (IEP). In Washington State, there are both informal and formal options. When parents and school districts are unable to work through disagreements, the procedural safeguards outline the dispute resolution processes available. These options ensure that parents and schools can work towards a mutually agreeable solution while protecting the child’s right to a Free Appropriate Public Education (FAPE). The formal dispute resolution options available through OSPI are mediation, due process hearings, and state complaints.
Disciplinary Protections
When disciplining students eligible for special education, schools must follow specific rules to ensure fair treatment. If a student is removed for more than 10 consecutive school days or shows a pattern of removals totaling over 10 days in a school year, it’s considered a change of placement, and parents must be notified. After 10 days, the school must provide services to help the student continue their education. A manifestation determination must be conducted within 10 days to see if the behavior was related to the student’s disability. If it was, the IEP team must address the behavior and return the student to their original placement unless agreed otherwise. If not, the student can be disciplined like other students but must still receive educational services.
Also, schools must keep providing educational services to students with disabilities even if they are removed from their current school setting for disciplinary reasons. This helps the student keep making progress in their education. Parents and guardians have the right to join meetings about their child’s disciplinary actions and can ask for a due process hearing if they disagree with decisions. These safeguards ensure students with disabilities receive necessary support and fair treatment during disciplinary actions.
In special cases, such as carrying a weapon or using drugs at school, the student can be placed in an alternative setting for up to 45 days regardless of whether the behavior was related to the student’s disability.
Protections for Students Not Yet Eligible for Special Education
The procedural safeguards outline protections for students who have not yet been found eligible for special education but for whom the school should have known needed services. A school is considered to have this knowledge if a parent previously expressed concerns in writing, requested an evaluation, or if staff raised concerns about the student’s behavior to supervisory personnel. However, if the parent refused an evaluation or the child was evaluated and found ineligible, the school is not considered to have knowledge. In these cases, the student may be disciplined like other students, but if an evaluation is requested during this period, it must be expedited. If the student is found eligible, special education services must be provided.
Requirements for Placement in Private Schools
If parents believe the public school cannot provide FAPE and choose to place their child in a private school, there are steps to request reimbursement from the district. If the child previously received special education services, a court or administrative law judge (ALJ) may require the district to reimburse the cost of private school enrollment if it is determined that the district did not timely provide FAPE and that the private placement is appropriate, even if it does not meet state educational standards.
Reimbursement may be reduced or denied if the parent did not inform the IEP team of their rejection of the proposed placement during the most recent IEP meeting, failed to provide written notice to the district at least 10 business days before the removal, or did not make the child available for a district evaluation after prior written notice. However, reimbursement cannot be denied if the district prevented the notice or if the parent was unaware of their responsibility to provide it. The court or ALJ may also choose not to reduce reimbursement if the parents are not able to read or write in English, or if reducing or denying the reimbursement would cause serious emotional harm to the child.
This PAVE article, Navigating Special Education in Private School, explains the rights of students to receive equitable services in private schools, regardless of whether they are placed there by their parents or through an Individualized Education Program (IEP) decision.
Procedural Safeguards under Section 504
The procedural safeguards under Section 504 ensure that parents are informed of their rights before any evaluation or development of a 504 plan begins. These safeguards include the right to request a referral for evaluation, the formation of a 504 team to assess the student’s needs, and the requirement for parental consent before any evaluation or implementation of the plan. Parents must be provided with a copy of their rights at key points in the process. Additionally, the school must review and evaluate the 504 plan annually and re-evaluate the student’s eligibility at least every three years. Parents also have the right to file formal complaints if they believe the school is not following the 504 plan or if their child is experiencing discrimination or harassment. The Section 504 Notice of Parent Rights is available for download in multiple languages from OSPI.
Conclusion
Procedural safeguards are a requirement under the Individuals with Disabilities Education Act (IDEA) that ensure the rights of students with disabilities and their parents are protected throughout the special education process. By outlining the legal protections available, these safeguards empower parents to actively participate in their child’s educational planning and decision-making. Understanding these rights—from prior written notice and parental consent to confidentiality and dispute resolution—allows families to advocate effectively and collaborate with schools. Through adherence to these safeguards, schools and parents can work together to provide a Free Appropriate Public Education (FAPE) tailored to the unique needs of each child.
Additional Resources:
- OSPI’s Special Education webpage includes information about data collection, dispute resolution, funding information, guidance for families, legal procedures, program improvement initiatives, resource libraries, and support for secondary transition services.
- Special Education Parent & Community Liaison provides non-legal support by phone (360-725-6075) or through an online message portal, Ask OSPI web page.
- PAVE provides direct support to parents and guardians, youth with disabilities, adult self-advocates, and professionals. Complete the Get Help request form to be connected with individualized information, resources, and training.
When Parents and Schools Disagree: Navigating Special Education Disputes
A Brief Overview:
- The Individuals with Disabilities Education Act (IDEA) requires states to provide ways to resolve disagreements between parents and schools about a student’s Individualized Education Program (IEP).
- IEP facilitation is a voluntary and informal process where a neutral facilitator helps parents and schools resolve special education concerns collaboratively. This service is provided at no cost by Sound Options Group.
- Washington State Governor’s Office of the Education Ombuds (OEO) acts as a neutral guide to help parents and schools resolve disagreements about special education services, without providing legal advice or advocacy.
- OSPI provides three formal special education dispute resolution processes: mediation, special education community complaint, and due process hearing.
- If parents win a due process hearing or civil lawsuit, the school district might have to pay their attorneys’ fees. Conversely, if the complaint is deemed frivolous, parents might have to pay the school district’s fees.
- Protections are in place for children not yet identified as needing special education if disciplinary actions are taken.
- Every school district has a process for filing complaints related to harassment, intimidation, and bullying (HIB).
- Complaints about discrimination involving students with disabilities can be filed with OSPI or the U.S. Department of Education’s Office for Civil Rights (OCR). OCR will not handle cases already being addressed by another agency or school process unless the process is completed and the complaint is filed within 60 days.
Full Article
The Individuals with Disabilities Education Act (IDEA) requires that each state education agency provide ways to solve disagreements between parents and schools regarding a student’s Individualized Education Program (IEP). These options ensure that parents and schools can work towards a mutually agreeable solution while protecting the child’s right to a Free Appropriate Public Education (FAPE). The Office of Superintendent of Public Instruction (OSPI) offers both informal and formal dispute resolution processes.
These dispute resolution options provide structured processes for addressing and resolving disagreements, ensuring that the rights of students with special needs are upheld and that they receive the education and services to which they are entitled.
Informal Dispute Resolution
IEP facilitation is a voluntary and informal process where parents and school districts can address their special education concerns with the assistance of a trained, neutral facilitator. This process allows both parties to resolve issues collaboratively without the formality of mediation, and it is provided at no cost. OSPI contracts with Sound Options Group to offer free facilitation services from facilitators skilled in conflict resolution to help clarify disputes, set agendas, and work towards mutually agreeable solutions. Participation in facilitation is entirely optional for both families and districts.
The IEP facilitation process starts when either a family or a school district contacts the Sound Options Group to request help. A parent can request facilitation by contacting Sound Options Group directly by phone at 800-692-2540 or 206-842-2298 (Seattle) to request a mediation session. For Washington State relay service, dial 800-833-6388 (TDD) or 800-833-6384 (voice). Sound Options Group gathers initial information about the student and the needs of both parties, confirming that both the family and district agree to proceed with a facilitated IEP meeting. Once the IEP team sets a date for the 3–4-hour meeting, the facilitator is assigned. The facilitator helps everyone prepare by sharing documents, setting a mutually agreeable agenda, confirming the meeting details, and preparing both parties for the meeting. After the facilitated IEP meeting, a case worker from Sound Options Group and the facilitator review the session and decide if another meeting is needed. A successful facilitated IEP meeting will result in the development of an IEP that is tailored to meet the unique needs of the student.
Another option for informal dispute resolution is Washington State Governor’s Office of the Education Ombuds (OEO), which helps parents and schools resolve disagreements about special education services. Acting as a neutral and independent guide, the OEO helps parents and educators understand special education regulations, facilitates problem-solving, and advises on communication strategies to support a team approach to a student’s education. The OEO does not provide legal advice, act as an attorney, conduct investigations, or advocate for any party. OEO can be contacted through their online intake form or by phone (1-866-297-2597) with language interpretation available.
Formal Dispute Resolution
When informal methods are unsuccessful, families and schools can turn to formal dispute resolution processes outlined in the procedural safeguards and available through the special education system. A copy of the procedural safeguards notice for Washington is downloadable in multiple languages from the Office of Superintendent of Public Instruction (OSPI).
In Washington state, the formal dispute resolution options are:
1. Mediation
Mediation is a voluntary process provided at no cost to parents and schools. It is designed to resolve disputes related to the identification, evaluation, educational placement, and provision of FAPE. Both parties must agree to participate in mediation. Mediators are trained, impartial individuals knowledgeable about special education laws. OSPI contracts with Sound Options Group to provide trained, neutral mediators to facilitate effective communication and problem-solving between parents and school districts. This brochure, Mediation in Special Education, outlines the services provided by Sound Options Group. Discussions during mediation are confidential and cannot be used in due process hearings or civil proceedings. If an agreement is reached, it must be documented in writing and is legally binding. Parents can contact Sound Options Group directly to request mediation.
2. Special Education Complaint
Any individual or organization can file a special education complaint if they believe a school district or public agency has violated Part B of the Individuals with Disabilities Education Act (IDEA). Complaints must be filed within one year of the alleged violation. OSPI investigates the complaint, gathering information from both the parent or guardian and the school district. OSPI then issues a written decision addressing the complaint and any corrective actions required within 60 days of receiving the complaint. PAVE has developed this training video, Procedural Safeguards: How to File a Special Education Complaint, that walks through OSPI’s community complaint form with a pretend scenario.
3. Due Process Hearing
A due process hearing is a formal meeting to resolve disputes about a child’s identification, evaluation, placement, or FAPE. Either parents or the school district can request this hearing, but they must do so within two years of the issue, unless there was misrepresentation or withheld information. The request for a due process hearing must be in writing, signed, and include:
- the name, address, and contact information of the student (even if homeless)
- the name of the student’s school
- the school district responsible for the IEP
- a description of the issue, the facts, and related events
- your proposed resolution
The original request must be provided to the other party – the parent or guardian must send it to the superintendent of the student’s school district, and the school district must provide the original to the parent or the guardian of the student. In addition, a copy of the request must be sent to the Office of Administrative Hearings by mail (PO Box 42489, Olympia, WA 98504-2489), fax (206-587-5135), or email (oah.ospi@oah.wa.gov). The party asking for a due process hearing must have proof that they gave their request to the other party.
Before the hearing, the school district must meet with the parents and relevant IEP team members within 15 days to try to resolve the issue at a resolution session. OSPI provides a direct to download form, Information and Forms on Resolution Sessions. During the hearing, both sides present evidence and witnesses. Parents have the right to bring a lawyer, present evidence, and question witnesses. An administrative law judge (ALJ) makes a decision, which can be appealed in state or federal court. The decision is final unless it is appealed and the decision is overturned. If an agreement is reached before the hearing, it must be written down in a settlement agreement.
For disputes about disciplinary actions that change a student’s placement, expedited due process hearings are available. These hearings happen faster than regular ones to resolve urgent issues quickly.
Dispute Resolution Outside of Special Education
If parents disagree with the decision made in a due process hearing, they have the right to file a civil lawsuit in state or federal court. This must be done within a specific time period, often 90 days, after the due process hearing decision. The court will review the administrative record, hear additional evidence if necessary, and make a ruling (decision) in the case. The civil lawsuit is not a part of the special education dispute resolution process and there are additional costs associated. Please note that PAVE is not a legal services agency and cannot provide legal advice or representation. Washington State Office of Administrative Hearings has compiled this Legal Assistance List for Special Education Due Process Disputes.
If parents win a due process hearing or lawsuit, the school district might have to pay their attorneys’ fees. But if the court decides the complaint was frivolous or filed for the wrong reasons, parents might have to pay the school district’s attorneys’ fees.
Additional Considerations
If a child hasn’t been identified as needing special education but parents think they should be, there are protections if the child faces disciplinary actions. If the school knew the child might need special education services before the behavior happened, they must follow special education disciplinary procedures.
Every school district has a process for filing a formal complaint related to harassment, intimidation and bullying (HIB). PAVE has compiled information and resources to address bullying in this article, Bullying at School: Resources and the Rights of Students with Special Needs.
Complaint Processes Related to Discrimination
OSPI’s Complaints and Concerns About Discrimination page states, “Each student must have equal access to public education without discrimination.” This page contains Discrimination Dispute Resolution Information Sheets that contain definitions of key terms, information about the role of district Civil Rights Compliance Coordinators, and instructions and requirements for filing different types of complaints, available for download in different languages. Anyone can file a complaint about discrimination involving students with disabilities in a Washington public school, which is prohibited by Washington law (RCW 28A.642.010). Formal discrimination complaints must be written, and the complaint must contain:
- a description of the incident
- why it is allegedly discriminatory
- proposed corrective action the district or charter school can take
The formal discrimination complaint must be hand carried, mailed, faxed, or emailed to district superintendent, administrator of the charter school, or Civil Rights Coordinator. When a school district or charter school receives a complaint, it must investigate and respond within 30 days, unless an extension is agreed upon. The civil rights coordinator provides the complaint procedure and ensures a thorough investigation. If exceptional circumstances require more time, the school must notify the complainant in writing. The school can also resolve the complaint immediately if both parties agree. After the investigation, the school must respond in writing, summarizing the results, stating whether they complied with civil rights law, explaining appeal options, and detailing any corrective measures, which must be implemented within 30 days unless otherwise agreed.
Students with disabilities in public schools are also protected against discrimination by federal laws, including Section 504 of the Rehabilitation Act of 1973 and IDEA. The U.S. Department of Education’s Office for Civil Rights (OCR) accept complaints with overlapping civil rights concerns, such as racism and disability discrimination. An OCR complaint must be filed within 180 calendar days of the alleged discrimination. If the school district’s dispute resolution process is already handling the case through a means like what OCR would provide, OCR will not take on the case. Once the school district’s process is completed, individuals have 60 days to file their complaint with OCR, which will then decide whether to accept the result from the other process. OCR provides step-by-step instructions for filing a discrimination complaint.
Some families are anxious about questioning actions taken by the school. Parents have protections under the law. The Office for Civil Rights maintains specific guidelines that prohibit retaliation against people who assert their rights through a complaint process.
Additional Resources:
- OSPI’s Dispute Resolution page
- OSPI’s Students’ Rights Information Sheet: Discriminatory Harassment (available in multiple languages)
- OSPI’s Students’ Rights Information Sheet: Section 504 (available in multiple languages)
- PAVE’s Quick Start Your Advocacy in Two Steps (video)
- TeamChild civil legal services provided to youth (King, Pierce, Spokane, and Yakima counties only)
What is a Medical Home?
Brief Overview
- A “medical home” is a coordinated care team with a coordinated care plan for an individual’s medical needs.
- Medical homes can be very useful any time an individual has more than one provider and more than one provider prescribing medications or treatments. They are not only for highly complex medical conditions.
- Medical homes have many advantages, but it’s important to select providers with the interest and qualities to make it work
- This article offers tips and questions to ask yourself and your family’s providers to help decide if your child or other family member needs a medical home.
Medical Home: What is it? Does my child need one?
- A medical home creates a coordinated team and a coordinated care plan around all your child’s medical needs. When a family or youth works with a physician or clinic to build (create) a medical home they all work together to “wrap around” the different medical providers and services needed for that person’s best health and wellbeing.
- Medical homes don’t happen right away and don’t always look the same. Often a medical home is started and/or managed through a primary care or pediatric clinic, but if a person has complex medical needs, a specialist provider, practice, or clinic may be a useful “site” for the medical home.
- Medical complexity, or a diagnosis that affects multiple systems in the body or has the potential to be life-threatening, adds its own set of challenges to a medical home. A medical home for an individual who is considered medically complex often has multiple specialists as well as therapists, medication management, and other systems such as school or early intervention. A good medical home can be a communication hub that helps this large multi-disciplinary team stay on the same page and not work at cross purposes.
- No matter who provides coordination, a medical home supports your child and helps you as the parent or guardian with care coordination. Some families have medical homes “built” through a specialist’s office, some a primary care pediatrician, and others who are on Medicaid can have that coordination through a managed care patient care specialist.
- There doesn’t need to be medical complexity to start discussing a medical home with a child’s team; there just needs to be more than one provider working with the child/youth or young adult, and with different medications prescribed by different providers. A medical home helps everyone be on the same page and you as a family to be part of the overall care plan.
- When working with a provider to develop a medical home, remember that respect is a two-way street. Working with complex needs can be frustrating and scary and just because someone is a physician doesn’t mean they have all the answers.
- Ask questions and let your providers know when you don’t understand a decision or if you disagree with their decision. This can be done respectfully and can help build a strong line of communication.
- A medical home set up under this mutual respect with the family and patient at the center and as co-creators of care is at the heart of the medical home idea and an essential foundation for a medical home that works.
When choosing a provider to help you create a medical home, here are questions to ask yourself:
- Who is being valued and honored as the expert on the child or youth? Is it the family and the individual?
- Is this team family and patient-centered?
- Is there trust and respect that goes both ways?
- Are Culture, race, language, and religion being honored?
- Is an effort being made to understand not only the diagnosis but also its long-term impact on the patient and the family?
- Are all an individual’s healthcare needs included in the care plan, including well-child and required immunizations?
- Can you get help to find specialty care and community services when needed?
- Do you feel supported in managing the care plan as a caregiver, family, or individual?
- Is information provided to help understand choices and options in care, and is time set aside for discussion, with the family and/or patient being the person who decides?
What other qualities are important when choosing a provider or practice to create a medical home?
- It’s helpful if your provider has at least some experience with the diagnosed condition. The relationship of the provider with a patient and their family can be just as important.
- Is the provider a good listener? Open communications are important so decisions are developed together, and the provider recognizes that the family and their youth/young adult are the experts in developing the young person’s care.
- If your child is a transitioning youth an important consideration may be a provider or clinic’s connection to adult care and their willingness to work with the youth rather than the adult caregiver in developing care plans.
- Does a provider work well with the other members of a child’s care team? Are they willing to communicate and think proactively about sharing information? When a family with their child, youth, or young adult works with a provider in a medical home to make decisions together as a team, and information is shared with all members of the team, it provides a robust model for long-term working care plan development no matter who moves in and out of that family and individual’s medical home.
- A willingness to work with supports inside and outside the medical profession is also something to think about. A physician that is willing to work with a school and advocate for the child’s needs in a school environment goes a long way in setting up a strong IEP or 504 education plan.
Additional advantages to consider taking time to work with a provider to develop a medical home:
- It can help in the early identification of additional healthcare needs or potential complications, creating a proactive approach
- Provides consistent, ongoing primary care
- Continuing coordination with a broad range of other specialty services
- Medical home team’s support can help in finding more medical services when needed
- More cost-effective care overall
- A child or youth’s doctors will get to know their needs and individual circumstances better
- The integrated partnership approach creates better healthcare outcomes
- Information is easier to share across the different providers, with therapists, schools, and the patient and families themselves
- Strong relationship building is emphasized in care
- Fewer visits to the emergency room and hospital when problems are found more quickly
Family can be a constant in many children’s lives. They know the history of the child and they will be there in the future.
Bringing a trusted medical provider into that circle to help with medical coordination and care can increase a family’s ability to look beyond the need to juggle the many issues of caring for a child with special healthcare needs.
A medical home can spread the burden of coordination and decision-making between many hands and can keep everyone on the same page. This alone can be worth the extra work that you may face in the beginning.
Resources
Here are some useful online resources for creating and using a medical home:
American Academy of Pediatrics
Related