Family caregivers for children with disabilities and special healthcare needs may feel isolated or uncertain about where to seek help for their children and themselves. A place for support is Parent to Parent (P2P), a network that connects families to trained parent volunteers who have experienced a similar journey with their own children. In addition to resources and information, parents share personal support and encouragement.
A Brief Overview
Full Article
Families new to the disability world can find preliminary information and request help right away by filling out a short form on a website page designed just for them, hosted by The Arc of Washington: Getting Started/Contact Us…Welcome to our World.
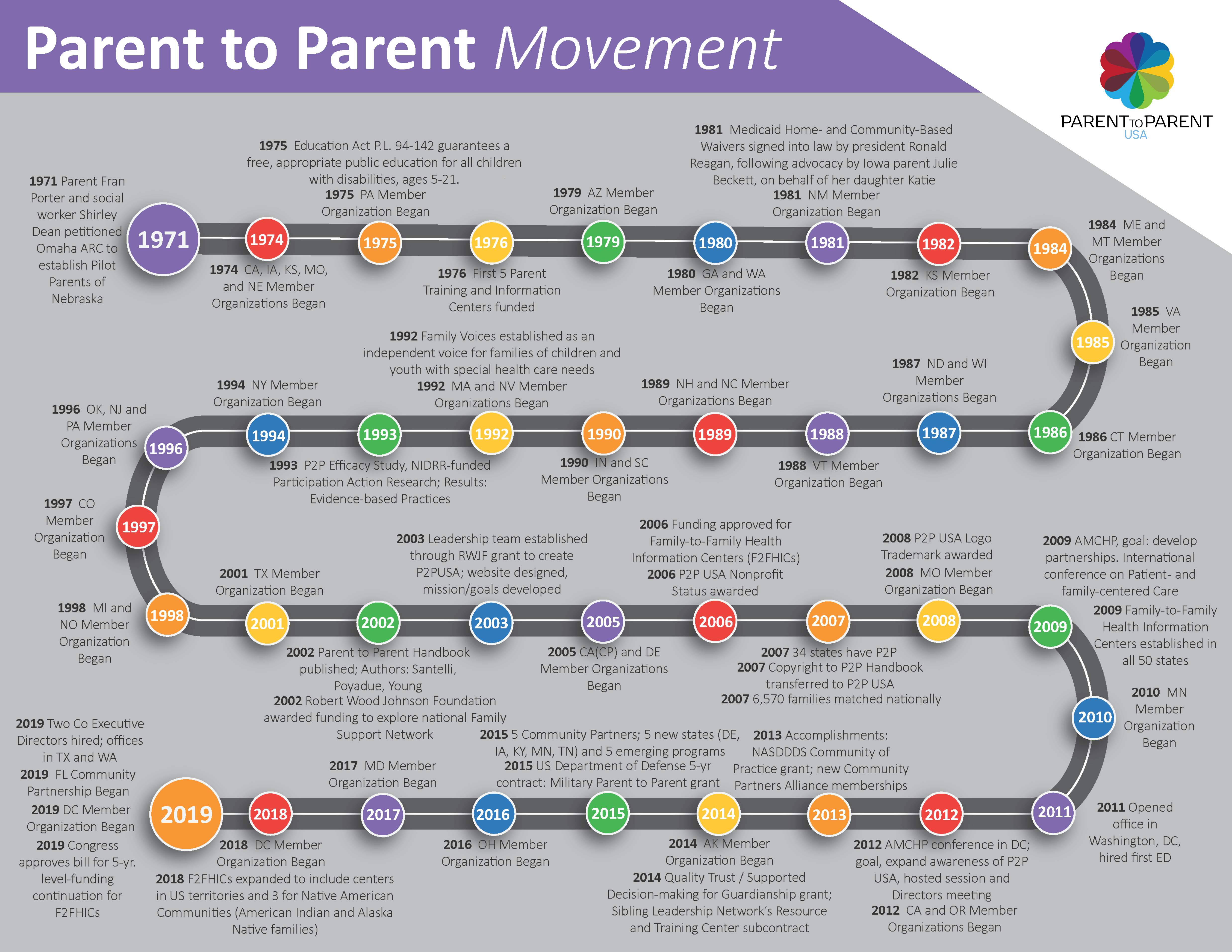
The first P2P program started in Nebraska in 1971. Programs started in Washington State in 1980. A national P2P network was established in 2003 to provide technical support to the statewide networks, with a goal to reach all 50 states. P2P USA provides an historical timeline.
Washington has a network of P2P programs that serve every corner of the state. The Arc provides support to the regional programs and links them to national P2P resources. Families can go to arcwa.org to find a list of P2P coordinators, organized by region and listed under the counties served.
¿Hablas español? Para más información y hacer referidos, llama a su condado abajo: Coordinadores de Enlance Hispano.
Families can request a parent match
When reaching out to the local P2P network, families can request a “parent match.” P2P leaders will locate a helping parent volunteer who has a similar lived experience and help the families get connected. From there, a supportive relationship can develop, where empathy, hope, and strength are shared.
Helping Parents cannot provide all answers, but they share insight, solidarity, and role modeling. They also share the joy and pride they’ve experienced while watching their child grow and achieve. A phrase commonly shared is: “I know, and I understand.”
In keeping with evidence-based practices promoted by national and state P2P organizations, the helping parent volunteers are training following a specific process and all personal information is kept confidential.
P2P services are free and include:
- Emotional support for family caregivers of children with special needs
- Referrals for community resources
- Information sharing about disabilities and medical conditions
- Family matching with trained helping parents
- Social and recreational events
- Training for parents who would like to become helping parent volunteers
- Disability awareness and community outreach
Someone to listen and understand
Washington’s statewide P2P is funded by The Arc of Washington State, the Developmental Disabilities Administration (DDA), and the Department of Health/Children with Special Health Care Needs. Individual county programs receive funding from host agencies, county DDA offices, the United Way, local grants, private donations, and more.
The Council for Exceptional Children published a research paper about P2P in 1999. Respondents to a national survey reported the following benefits from participating in P2P:
- Someone to listen and understand (66 percent)
- Disability information (63 percent)
- Care for my child (58 percent
- Ways to find services (54 percent)
Statewide, various agencies and family-led organizations host local P2P programs. An interactive map of Washington State provides an easy way to locate information in English and Spanish about a P2P program in your area.
Another way to begin is to contact the statewide P2P coordinator, Tracie Hoppis, by sending an email to: parent2parentwa@arcwa.org.




{kind=link}